
Page 79 - 2023 SMOG Digital
P. 79
CBRN
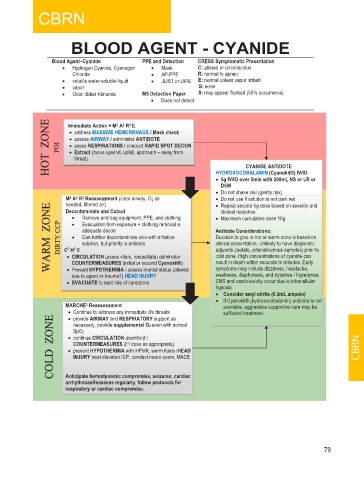
BLOOD AGENT - CYANIDE
Blood Agent–Cyanide PPE and Detection CRESS Symptomatic Presentation
• Hydrogen Cyanide, Cyanogen • Mask C: altered or unconscious
Chloride • AP-PPE R: normal to apneic
• volatile water-soluble liquid • JLIST or UIPE E: normal unless vapor irritant
• vapor S: none
• Odor: Bitter Almonds M8 Detection Paper S: may appear flushed (50% occurrence)
• Does not detect
HOT ZONE POI Immediate Action + M 2 A 2 R 2 E.
• address MASSIVE HEMORRHAGE / Mask check
• assess AIRWAY / administer ANTIDOTE
• asses RESPIRATIONS / conduct RAPID SPOT DECON
• Extract (move upwind, uphill, upstream – away from
threat)
CYANIDE ANTIDOTE
HYDROXOCOBALAMIN (Cyanokit®) IV/IO
• 5g IV/IO over 5min with 200mL NS or LR or
L
D5W
• Do not shake vial (gently mix)
M 2 A 2 R 2 Reassessment (clear airway, O 2 as • Do not use if solution is not dark red
s
s
WARM ZONE DIRTY CCP C H E Remove and bag equipment, PPE, and clothing • Maximum cumulative dose 10g
needed, filtered air)
• Repeat second 5g dose based on severity and
Decontaminate and Cutout
clinical response
•
Evacuation from exposure + clothing removal is
•
adequate decon
Antidote Considerations:
Can further decontaminate skin with irritation
Decision to give in hot or warm zone is based on
•
solution, but priority is antidote
clinical presentation. Unlikely to have diagnostic
adjuncts (lactate, arterial/venous samples) prior to
2
2
cold zone. High concentrations of cyanide can
• CIRCULATION (asses vitals, resuscitate) administer
COUNTERMEASURES (initial or second Cyanokit®)
symptoms may include dizziness, headache,
• Prevent HYPOTHERMIA / assess mental status (altered
weakness, diaphoresis, and dyspnea / hyperpnea.
due to agent or trauma?) HEAD INJURY result in death within seconds to minutes. Early
• EVACUATE to next role of care/zone CNS and cardiotoxicity occur due to intracellular
hypoxia.
• Consider amyl nitrite (0.3mL ampule)
• If Cyanokit® (hydroxocobalamin) antidote is not
MARCHE 2 Reassessment available, aggressive supportive care may be
• Continue to address any immediate life threats sufficient treatment.
COLD ZONE • continue CIRCULATION (monitor)t / CBRN
• provide AIRWAY and RESPIRATORY support as
necessary, provide supplemental O2 even with normal
SpO2
COUNTERMEASURES 2 nd dose as appropriate)
• prevent HYPOTHERMIA with HPMK, warm fluids /HEAD
INJURY treat elevated ICP, conduct neuro exam, MACE
Anticipate hemodynamic compromise, seizures, cardiac
arrhythmiasReassess regularly, follow protocols for
respiratory or cardiac compromise.
79