
Page 40 - JSOM Spring 2025
P. 40
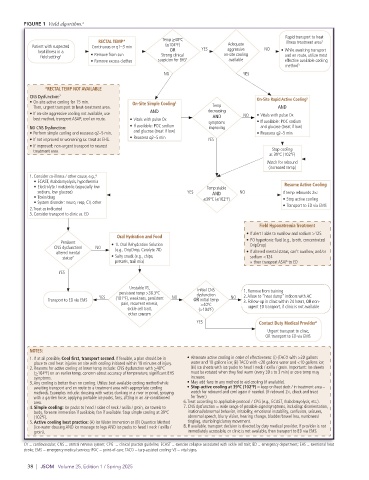
FIGURE 1 Field algorithm. 1
Rapid transport to heat
RECTAL TEMP* Temp ≥40ºC illness treatment area 1
Patient with suspected Continuous or q1–3 min (≥104ºF) YES Adequate NO
aggressive
heat illness in a OR on-site cooling • While awaiting transport
field setting 1 • Remove from sun Strong clinical and en route, utilize most
• Remove excess clothes suspicion for EHS 2 available effective available cooling
method 3
NO YES
*RECTAL TEMP NOT AVAILABLE
CNS Dysfunction: 7 On-Site Rapid Active Cooling 5
• On-site active cooling for 15 min. On-Site Simple Cooling 4
Then, urgent transport to heat-treatment area. Temp AND
• If on-site aggressive cooling not available, use AND decreasing NO • Vitals with pulse Ox
AND
best method, transport ASAP, cool en route. • Vitals with pulse Ox symptoms • If available: POC sodium
NO CNS Dysfunction: • If available: POC sodium improving and glucose (treat if low)
• Perform simple cooling and reassess q2–5 min. and glucose (treat if low) • Reassess q2–5 min
• If not improved or worsening sx: treat as EHS. • Reassess q2–5 min YES
• If improved: non-urgent transport to nearest
treatment area. Stop cooling
at 39ºC (102ºF)
Watch for rebound
(increased temp)
1. Consider co-illness / other cause, e.g., 6
• ECAST, rhabdomyolysis, hypothermia
• Electrolyte / metabolic (especially low Temp stable Resume Active Cooling
sodium, low glucose) YES AND NO If temp rebounds 2×:
• Toxin/drug ≤39ºC (≤102ºF) • Stop active cooling
• System disorder: neuro, resp, CV, other
2. Treat as indicated • Transport to ED via EMS
3. Consider transport to clinic vs. ED
Field Hyponatremia Treatment
• If alert / able to swallow and sodium >125
Oral Hydration and Food
Persisent • 1L Oral Rehydration Solution • PO hypertonic fluid (e.g., broth, concentrated
CNS dysfunction/ NO (e.g., DripDrop, Ceralyte 70) DripDrop)
altered mental • If altered mental status, can’t swallow, and/or
status 7 • Salty snack (e.g., chips, sodium <124
pretzels, trail mix) o then transport ASAP to ED
YES
Unstable VS, Initial CNS
persistent temp >38.3ºC dysfunction 1. Remove from training
YES (101ºF), weakness, persistent NO NO 2. Allow to “heat dump” indoors with AC
Transport to ED via EMS OR initial temp 3. Follow-up in clinic within 24 hours, OR non-
pain, recurrent emesis, >40ºC
sickle cell trait, (>104ºF) urgent ED transport, if clinic is not available
other concern
YES Contact Duty Medical Provider 8
Urgent transport to clinic,
OR transport to ED via EMS
NOTES:
1. If at all possible, Cool first, transport second. If feasible, a plan should be in • Alternate active cooling in order of effectiveness: (i) (TACO with >20 gallons
place to cool heat injuries on site with cooling initiated within 10 minutes of injury. water and 10 gallons ice; (ii) TACO with <20 gallons water and <10 gallons ice;
2. Reasons for active cooling at lower temp include: CNS dysfunction with >40ºC (iii) ice sheets with ice packs to head / neck / axilla / groin. Important: Ice sheets
(>104ºF) on an earlier temp, concern about accuracy of temperature, significant EHS must be rotated when they feel warm (every 30 s to 3 min) or core temp may
symptoms. increase.
3. Any cooling is better than no cooling. Utilize best available cooling method while • May add fans to any method to aid cooling (if available).
awaiting transport and en route to a treatment area with appropriate cooling • Stop active cooling at 39ºC (102ºF) – keep on heat deck / in treatment area –
methods. Examples include: dousing with water, dunking in a river or pond, spraying watch for rebound and cool again if needed. (If rebound 2×, check and treat
with a garden hose, applying portable ice packs, fans, sitting in an air-conditioned for fever.)
area. 6. Treat according to applicable protocol / CPG (e.g., ECAST, rhabdomyolysis, etc.).
4. Simple cooling: Ice packs to head / sides of neck / axilla / groin, ice towels to 7. CNS dysfunction = wide range of possible signs/symptoms, including: disorientation,
body, forearm immersion if available, fan if available. Stop simple cooling at 39ºC irrational/abnormal behavior, irritability, emotional instability, confusion, seizures,
(102ºF). abnormal speech, blurry vision, hearing change, bladder/bowel loss, numbness/
5. Active cooling best practice: (A) Ice Water Immersion or (B) Quantico Method tingling, stumbling/clumsy movement.
(ice-water dousing AND ice massage to legs AND ice packs to head / neck / axilla / 8. If available, transport decision is directed by duty medical provider. If provider is not
groin). immediately accessible, or clinic is not available, then transport to ED via EMS.
CV = cardiovascular; CNS = central nervous system; CPG = clinical practice guideline; ECAST = exercise collapse associated with sickle cell trait; ED = emergency department; EHS = exertional heat
stroke; EMS = emergency medical services; POC = point-of-care; TACO = tarp-assisted cooling; VS = vital signs.
38 | JSOM Volume 25, Edition 1 / Spring 2025