
Page 44 - JSOM Winter 2024
P. 44
As shown in Table 1, the median age was 26 (interquartile TABLE 2 Concomitant Prehospital Interventions
range [IQR] 21–31) years, and all were men. The most fre- No. (%) of cases;
quent recipients were partner force (28%), followed by U.S. Intervention n=39
military (26%). The most common mechanisms of injury were Airway adjunct 4 (10)
explosives (59%), followed by firearms (38%). The median Cricothyrotomy 1 (3)
composite injury severity score was 10 (IQR 5–18). The most
common sites of serious injury (AIS >3) were the extremities Blood product 6 (15)
(58%), followed by the abdomen (10%) and skin (10%). Only Intraosseous access 7 (18)
one casualty did not survive. Intravenous fluids 11 (28)
Limb tourniquet 16 (41)
TABLE 1 Casualty Characteristics Tranexamic acid 8 (21)
No. (%) of cases*; Warming 21 (54)
Characteristic n=39 Hemostatic dressing 8 (21)
Demographics
Age, median (IQR) 26 (21–31) TABLE 3 24-Hour Blood and Fluid Consumption
Men 39 (100) Mean volume
Affiliation Fluid (95% CI)
U.S. military 10 (26) Crystalloid and colloid, mL 1,200 (0–6,116)
U.S. contractor 1 (3) Whole blood, U 0 (0–1)
Partner forces 11 (28) Packed red blood cells, U 3 (0–8)
Humanitarian 17 (44) Platelets, U 0 (0–1)
Mechanism of injury Cryoprecipitate, U 0 (0–0)
Explosive 23 (59 ) Plasma, U 2 (0–6)
Firearm 15 (38 )
Other 1 (3) TABLE 4 Select Associated Injury Diagnoses
Composite injury severity score, median (IQR) 10 (5–18) No. (%) of cases;
Serious injury by body region Diagnosis n=39
Head/neck 3 (8) Lower extremity amputation 24 (62)
Face 0 (0) Testis avulsion or amputation 11 (28)
Thorax 5 (13) Pelvic fracture 9 (23)
Abdomen 4 (10) Tympanic membrane rupture 9 (23)
Extremities 21 (54) Colonic laceration 7 (18)
Skin 4 (10) Upper extremity amputation 6 (15)
Outcome Brachial artery laceration 6 (15)
Alive at discharge 38 (97) Femoral artery laceration 5 (13)
*Unless otherwise specified. Concussion 4 (10)
IQR = interquartile range.
TABLE 5 Select Associated Hospital Procedures
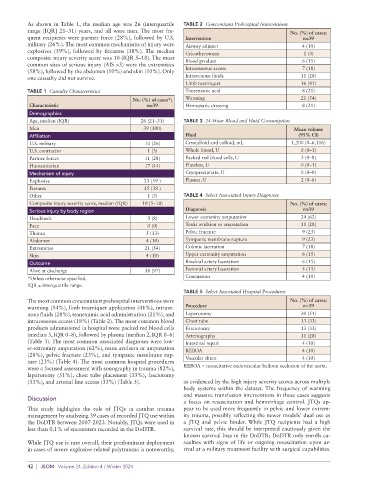
The most common concomitant prehospital interventions were No. (%) of cases;
warming (54%), limb tourniquet application (41%), intrave- Procedure n=39
nous fluids (28%), tranexamic acid administration (21%), and Laparotomy 20 (51)
intraosseous access (18%) (Table 2). The most common blood Chest tube 13 (33)
products administered in hospital were packed red blood cells Fasciotomy 13 (33)
(median 3, IQR 0–8), followed by plasma (median 2, IQR 0–6) Arteriography 11 (28)
(Table 3). The most common associated diagnoses were low- Intestinal repair 4 (10)
er-extremity amputation (62%), testis avulsion or amputation REBOA 4 (10)
(28%), pelvic fracture (23%), and tympanic membrane rup-
ture (23%) (Table 4). The most common hospital procedures Vascular shunt 4 (10)
were a focused assessment with sonography in trauma (82%), REBOA = resuscitative endovascular balloon occlusion of the aorta.
laparotomy (51%), chest tube placement (33%), fasciotomy
(33%), and arterial line access (33%) (Table 5). as evidenced by the high injury severity scores across multiple
body systems within the dataset. The frequency of warming
and massive transfusion interventions in these cases suggests
Discussion
a focus on resuscitation and hemorrhage control. JTQs ap-
This study highlights the role of JTQs in combat trauma pear to be used more frequently in pelvic and lower extrem-
management by analyzing 39 cases of recorded JTQ use within ity trauma, possibly reflecting the newer models’ dual use as
the DoDTR between 2007-2023. Notably, JTQs were used in a JTQ and pelvic binder. While JTQ recipients had a high
less than 0.1% of encounters recorded in the DoDTR. survival rate, this should be interpreted cautiously given the
known survival bias in the DoDTR; DoDTR only enrolls ca-
While JTQ use is rare overall, their predominant deployment sualties with signs of life or ongoing resuscitation upon ar-
in cases of severe explosive-related polytrauma is noteworthy, rival at a military treatment facility with surgical capabilities.
42 | JSOM Volume 24, Edition 4 / Winter 2024