
Page 67 - JSOM Spring 2020
P. 67
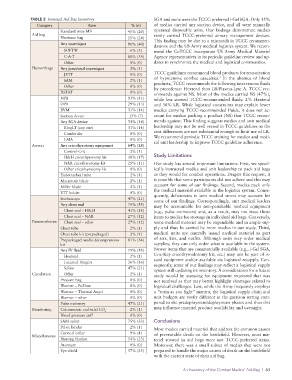
TABLE 2 Itemized Aid Bag Inventory SGA and none were the TCCC-preferred i-Gel SGA. Only 15%
Category Item % (n) of medics carried any suction device, and all were manually
Standard issue M9 45% (20) operated disposable units. Our findings demonstrate medics
Aid bag rarely carried TCCC-preferred airway management devices.
Nonissue bag 55% (24) This finding may be due to a mismatch in TCCC recommen-
Any tourniquet 91% (40) dations and the US Army medical logistics system. We recom-
SOFTW 6% (3) mend the CoTCCC incorporate US Army Medical Materiel
C-A-T 88% (39) Agency representatives in its periodic guideline review and up-
Other 0% (0) dates to synchronize the medical and logistical communities.
Hemorrhage Any junctional tourniquet 2% (1)
JETT 0% (0) TCCC guidelines recommend blood products for resuscitation
of hypotensive combat casualties. In the absence of blood
2
SAM 2% (1) products, TCCC recommends the following intravenous fluids
Other 0% (0) by precedence: Hextend then LR/Plasma-Lyte A. TCCC rec-
XSTAT 0% (0) ommends against NS. Most of the medics carried NS (47%),
NPA 93% (41) while less stowed TCCC-recommended fluids: 2% Hextend
OPA 29% (13) and 36% LR. While logistical constraints may explain fewer
BVM 31% (14) medics carrying TCCC-recommended fluids, it does not ac-
Suction device 15% (7) count for medics packing a product (NS) that TCCC recom-
Any SGA device 31% (14) mends against. This finding suggests medics and unit medical
KingLT (any size) 31% (14) leadership may not be well versed in TCCC guidelines as the
Combitube 0% (0) cost differences are not substantial enough to limit use of LR.
We recommend periodic TCCC training for medics and medi-
LMA 0% (0) cal unit leadership to improve TCCC guideline adherence.
Airway Any cricothyrotomy equipment 64% (28)
Control-Cric 2% (1)
H&H cricothyrotomy kit 38% (17) Study Limitations
NAR cricothyrotomy kit 25% (11) Our study has several important limitations. First, we specif-
Other cricothyrotomy kit 0% (0) ically instructed medics and unit leadership to pack aid bags
Endotracheal tube 2% (1) as they would for combat operations. Despite this request, it
Macintosh blade 2% (1) is possible that some participants did not adhere and this may
Miller blade 2% (1) account for some of our findings. Second, medics pack only
the medical materiel available in the logistics system. Conse-
ETT holder 0% (0) quently, deficiencies in unit medical stores may account for
Stethoscope 47% (21) some of our findings. Correspondingly, unit medical leaders
Any chest seal 75% (33) may be accountable for non-perishable medical equipment
Chest seal – H&H 41% (18) (e.g., pulse oximeters) and, as a result, may not issue those
Chest seal – NAR 27% (12) items to medics for stowage in individual aid bags. Conversely,
Pneumothorax Chest seal – other 27% (12) some medical materiel may be expendable and in ample sup-
Chest tube 2% (1) ply and thus be carried by more medics in our study. Third,
Chest tube kit (prepackaged) 2% (1) medical units are centrally issued medical materiel as part
Prepackaged needle decompression 81% (36) of sets, kits, and outfits. Although units may order medical
kit supplies, they can only order what is available in the system.
Any IV fluid 75% (33) Newer items that are commercially available (e.g., i-Gel SGA,
Hextend 2% (1) Cric-Key cricothyroidotomy kit, etc.) may not be part of is-
sued equipment and/or available via logistical resupply. Con-
Lactated Ringers 36% (16) sequently, some of our findings may reflect a logistical supply
Saline 47% (21) system still updating its inventory. A consideration for a future
Circulation Other 2% (1) study would be assessing for equipment requested that was
Pressure bag 0% (0) not received as that may better highlight shortages related to
Warmer – EnFlow 0% (0) logistical challenges. Last, while the Army frequently employs
Warmer – Thermal Angel 0% (0) a “train as you fight” mantra, the logistical supply chain and
Warmer – other 0% (0) unit budgets are vastly different in the garrison setting com-
Pulse oximetry 47% (21) pared to the predeployment/deployment phases and thus this
Monitoring Colorimetric end-tidal CO 2% (1) may influence materiel product availability and oversight.
2
Blood pressure cuff 0% (0)
SAM splint 75% (33) Conclusions
Pelvic binder 2% (1) Most medics carried materiel that address the common causes
Cervical collar 9% (4) of preventable death on the battlefield. However, most ma-
Miscellaneous
Heating blanket 54% (23) teriel stowed in aid bags were not TCCC-preferred items.
Atomizer 0% (0) Moreover, there was a small subset of medics that were not
Eye shield 57% (25) prepared to handle the major causes of death on the battlefield
with the current state of their aid bag.
An Inventory of the Combat Medics’ Aid Bag | 63