
Page 73 - JSOM Summer 2019
P. 73
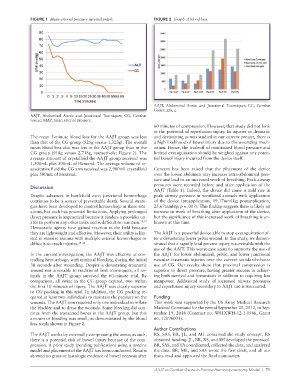
FIGURE 1 Mean arterial pressure survival graph. FIGURE 2 Graph of blood loss.
AAJT, Abdominal Aortic and Junctional Tourniquet; CG, Combat
Gauze; gm, g.
AAJT, Abdominal Aortic and Junctional Tourniquet; CG, Combat
Gauze; MAP, mean arterial pressure.
60 minutes of compression. However, that study did not look
at the potential of reperfusion injury. In injuries as dramatic
The mean 5-minute blood loss for the AAJT group was less and devastating as was studied in our current project, there is
than that of the CG group (525g versus 1,323g). The overall a high likelihood of bowel injury due to the wounding mech-
mean blood loss also was less in the AAJT group than in the anism. Hence, the tradeoff of maintained blood pressure and
CG group (918g versus 2,718g, respectively; Figure 2). The limited exsanguination should be weighed against any poten-
average amount of crystalloid the AAJT group received was tial bowel injury incurred from the device itself.
1,300mL plus 500mL of Hextend. The average volume of re-
suscitative fluid the CG arm received was 2,900mL crystalloid Concern has been raised that the placement of the device
plus 500mL of Hextend. over the lower abdomen may increase intra-abdominal pres-
sure and lead to an increased work of breathing. Peak airway
pressures were recorded before and after application of the
Discussion
AAJT (Table 1). Indeed, the device did cause a mild rise in
Despite advances in battlefield care, junctional hemorrhage peak airway pressure in ventilated animals with application
continues to be a source of preventable death. Several strate- of the device (preapplication, 19.17mmHg; postapplication,
gies have been developed to control hemorrhage in these situ- 25.67mmHg; p = .007). This finding suggests there is likely an
ations, but each has potential limitations. Applying prolonged increase in work of breathing after application of the device,
direct pressure is impractical because it renders a provider un- but the significance of this increased work of breathing is un-
able to perform any other tasks and is difficult to maintain. 15,17 known at this time.
Hemostatic agents have gained traction in the field because
they are lightweight and effective. However, their utility is lim- The AAJT is a powerful device able to stop exsanguination af-
ited in massive trauma with multiple arterial hemorrhages or ter a devastating lower pelvis wound. In this study, we demon-
difficult-to-reach injuries. 18–22 strated that a rapidly fatal porcine injury is survivable with the
use of the AAJT. This worst-case scenario supports the use of
In the current investigation, the AAJT was effective at con- the AAJT for lower abdominal, pelvic, and lower junctional
trolling hemorrhage, with minimal bleeding, during the initial vascular traumatic injuries over the current standard-of-care
30 seconds after wounding. Despite a devastating traumatic use of CG. Our results show that proximal compression is
wound not amenable to traditional limb tourniquets, all an- superior to direct pressure, having greater success in achiev-
imals in the AAJT group survived the 60-minute trial. By ing both survival and hemostasis in addition to requiring less
comparison, all swine in the CG group expired, two within manpower. Additional study of increased airway pressures
the first 10 minutes of injury. The AAJT was clearly superior and reperfusion injury secondary to AAJT use is warranted.
to CG packing in this trial. In addition, the CG packing re-
quired at least two individuals to maintain the pressure on the Funding
wounds. The AAJT arm required only one individual to inflate This work was supported by the US Army Medical Research
the bladder and to dress the wounds. Some bleeding did con- Material Command for the period September 20, 2012, to Sep-
tinue from the transected bones in the AAJT group, but this tember 19, 2014 (Contract no. W81XWH-12-1-0546, Grant
amount of bleeding was small, as demonstrated by the blood no. 12096001).
loss totals shown in Figure 2.
Author Contributions
The AAJT works by externally compressing the aorta; as such, RS, SAS, BR, JL, and ML conceived the study concept. RS
there is a potential risk of bowel injury because of the com- obtained funding. JL, BR, RS, and SH developed the protocol.
pression. A prior study (pending publication) using a porcine BR, SAS, and TA coordinated, collected the data, and analyzed
model and placement of the AAJT has been conducted. Results the data. BR, ML, and SAS wrote the first draft, and all au-
showed no gross or histologic evidence of bowel necrosis after thors read and approved the final manuscript.
AAJT vs Combat Gauze in Porcine Hemicorporectomy Model | 71