
Page 56 - JSOM Summer 2018
P. 56
of moxifloxacin orally for all patients with penetrating eye on arrival, and three were enemy prisoners of war; data from
trauma or other open combat wounds who are able to take oral these casualties were excluded. Of the remaining 705 casual-
medications. For patients with penetrating eye trauma or open ties with available records, 643 (91.2%) had battle injuries,
combat wounds unable to take oral medication (owing to, for and there were 550 with a documented open wound, including
example, shock, unresponsive, or abdominal injury), TCCC penetrating eye injury, other penetrating trauma, amputation,
guidelines recommend ertapenem 1g IV or IM once daily. 10,11 laceration, degloving, or gunshot wound (Table 1). Within the
550, 30 (5.5%) had a concomitant penetrating eye injury. Four
The current TCCC guidelines have made recommendations of the 30 (13.3%) were noted to have bilateral eye wounds. Of
for the use of antibiotic medications for the prehospital pro- the 550 casualties with documented open wounds, 93 (16.9%)
viders at the point of injury. Prehospital provider adherence were conventional forces, 100 (18.2%) were Special Opera-
with this recommendation is unclear. The aim of this study tions Command forces, 323 (58.7%) were Afghan-component
was to evaluate adherence to TCCC guidelines for prehospital forces (e.g., military, policy), and 34 (6.2%) were civilian or
medication administration, specifically for antibiotics for open unknown. Table 2 outlines the causes of the injury. There
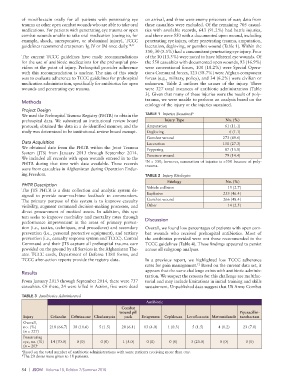
wounds and penetrating eye trauma. were 327 total instances of antibiotic administration (Table
3). Given that many of these injuries were the result of poly-
trauma, we were unable to perform an analysis based on the
Methods
etiology of the injury or the injuries sustained.
Project Design
We used the Prehospital Trauma Registry (PHTR) to obtain the TABLE 1 Injuries Sustained a
prehospital data. We submitted an institutional review board Injury Type No. (%)
protocol; obtained the data in a de-identified manner; and the Amputation 61 (11.1)
study was determined to be institutional review board exempt. Degloving 6 (1.1)
Gunshot wound 273 (49.6)
Data Acquisition Laceration 150 (27.3)
We obtained data from the PHTR within the Joint Trauma Peppering 87 (15.8)
System (JTS) from January 2013 through September 2014.
We included all records with open wounds entered in to the Puncture wound 79 (14.4)
PHTR during that time with data available. These records a N = 550; however, summation of injuries is >550 because of poly-
were from casualties in Afghanistan during Operation Endur- trauma.
ing Freedom. TABLE 2 Injury Etiologies
Etiology No. (%)
PHTR Description Vehicle collision 15 (2.7)
The JTS PHTR is a data collection and analytic system de-
signed to provide near–real-time feedback to commanders. Explosive 255 (46.4)
The primary purpose of this system is to improve casualty Gunshot wound 266 (48.4)
visibility, augment command decision-making processes, and Other 14 (2.5)
direct procurement of medical assets. In addition, this sys-
tem seeks to improve morbidity and mortality rates through
performance improvement in the areas of primary preven- Discussion
tion (i.e., tactics, techniques, and procedures) and secondary Overall, we found low percentages of patients with open com-
prevention (i.e., personal protective equipment), and tertiary bat wounds who received prehospital antibiotics. Most of
prevention (i.e., casualty response system and TCCC). Central the antibiotics provided were not those recommended in the
Command and their JTS capture all prehospital trauma care TCCC guidelines (Table 4). These findings appeared to persist
provided on the ground by all Services in the Afghanistan The- across all subgroup analyses.
ater. TCCC cards, Department of Defense 1380 forms, and
TCCC after-action reports provide the registry data. In a previous report, we highlighted low TCCC adherence
rates for pain management. Based on the current data set, it
12
Results appears that the same challenge exists with antibiotic adminis-
tration. We suspect the reasons for this challenge are multifac-
From January 2013 through September 2014, there were 737 torial and may include limitations in initial training and skills
casualties. Of these, 24 were killed in Action, five were dead sustainment. Unpublished data suggest that US Army Combat
TABLE 3 Antibiotics Administered
Antibiotic
Combat
wound pill Piperacillin-
Injury Cefazolin Ceftriaxone Clindamycin pack Ertapenem Cephlexan Levofloxacin Metronidazole tazobactam
Overall,
no. (%) 218 (66.7) 38 (11.6) 5 (1.5) 20 (6.1) 13 (4.0) 1 (0.3) 5 (1.5) 4 (1.2) 23 (7.0)
(n = 327)
Penetrating
eye, no. (%) 14 (70.0) 0 (0) 0 (0) 1 (5.0) 0 (0) 0 (0) 5 (25.0) 0 (0) 0 (0)
(n = 20) b
a Based on the total number of antibiotic administrations with some patients receiving more than one.
b The 20 doses were given to 18 patients.
54 | JSOM Volume 18, Edition 2/Summer 2018