
Page 45 - JSOM Winter 2017
P. 45
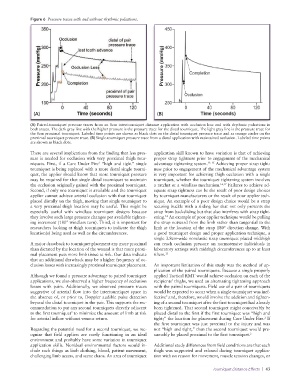
Figure 6 Pressure traces with and without rhythmic pulsations.
(A) (B)
(A) Paired-tourniquet pressure traces from an 8cm intertourniquet distance application with occlusion loss and with rhythmic pulsations in
both traces. The dark gray line with the higher pressure is the pressure trace for the distal tourniquet. The light gray line is the pressure trace for
the 8cm proximal tourniquet. Labeled time points are shown as black dots on the distal tourniquet pressure trace and as orange circles on the
proximal tourniquet pressure trace. (B) Single-tourniquet pressure trace from a distal application with maintained occlusion. Labeled time points
are shown as black dots.
There are several implications from the finding that less pres- application skill known to have variation is that of achieving
sure is needed for occlusion with very proximal thigh tour- proper strap tightness prior to engagement of the mechanical
2
niquets. First, if a Care Under Fire “high and tight” single advantage tightening system. 13–15 Achieving proper strap tight-
tourniquet is being replaced with a more distal single tourni- ness prior to engagement of the mechanical advantage system
quet, the applier should know that more tourniquet pressure is very important for achieving thigh occlusion with a single
may be required for that single distal tourniquet to maintain tourniquet, whether the tourniquet tightening system involves
the occlusion originally gained with the proximal tourniquet. a ratchet or a windlass mechanism. 16,17 Failures to achieve ad-
Second, if only one tourniquet is available and the tourniquet equate strap tightness can be the result of poor design choices
applier cannot achieve arterial occlusion with that tourniquet by tourniquet manufacturers or the result of poor applier tech-
placed distally on the thigh, moving that single tourniquet to nique. An example of a poor design choice would be a strap
a very proximal thigh location may be useful. This might be securing buckle with a sliding bar that not only prevents the
especially useful with windlass tourniquet designs because strap from backsliding but that also interferes with strap tight-
14
they involve such large pressure changes per available tighten- ening. An example of poor applier technique would be pulling
ing increment (180° windlass turn). Third, it is important for the strap outward from the limb rather than tangential to the
researchers looking at thigh tourniquets to indicate the thigh limb at the location of the strap 180° direction change. With
location(s) being used as well as the circumferences. a good tourniquet design and proper application technique, a
single 3.8cm-wide nonelastic strap tourniquet placed midthigh
A major drawback to tourniquet placement any more proximal can reach occlusion pressure on normotensive individuals in
than dictated by the location of the wound is that more proxi- laboratory settings with midthigh circumferences up to at least
mal placement puts more limb tissue at risk. Our data indicate 63cm. 13
that an additional drawback may be a higher frequency of oc-
clusion losses with increasingly proximal tourniquet placement. An important limitation of this study was the method of ap-
plication of the paired tourniquets. Because a single properly
Although we found a pressure advantage to paired tourniquet applied Tactical RMT would achieve occlusion on each of the
applications, we also observed a higher frequency of occlusion recipients’ thighs, we used an alternating tightening approach
losses with pairs. Additionally, we observed pressure traces with the paired tourniquets. Field use of a pair of tourniquets
suggestive of arterial flow into the intertourniquet space in would be expected to occur when a single tourniquet was inef-
2
the absence of, or prior to, Doppler audible pulse detection fective and, therefore, would involve the addition and tighten-
beyond the distal tourniquet in the pair. This supports the rec- ing of a second tourniquet after the first tourniquet had already
ommendation to put any second tourniquets directly adjacent been tightened. That second tourniquet might conceivably be
to the first tourniquet to minimize the amount of limb at risk placed distal to the first if the first tourniquet was “high and
2
for arterial inflow without venous return. tight;” the location for placement during Care Under Fire. If
2
the first tourniquet was just proximal to the injury and was
Regarding the potential need for a second tourniquet, we rec- not “high and tight,” then the second tourniquet would pre-
ognize that field appliers are rarely functioning in an ideal sumably be placed proximal to the first tourniquet. 2
environment and probably have some variation in tourniquet
application skills. Nonideal environmental factors would in- Additional study differences from field conditions are that each
clude such things as limb clothing, blood, patient movement, thigh was supported and relaxed during tourniquet applica-
challenging limb access, and scene chaos. An area of tourniquet tion with no reason for movement, muscle tension changes, or
Tourniquet Distance Effects | 43