
Page 100 - JSOM Winter 2017
P. 100
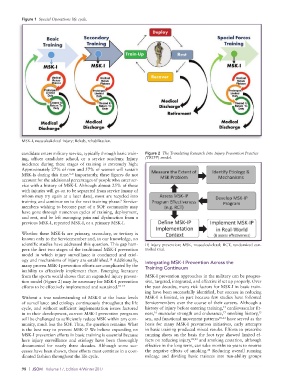
Figure 1 Special Operations life cycle.
MSK-I, musculoskeletal injury; Rehab, rehabilitation.
candidate enters military service, typically through basic train- Figure 2 The Translating Research Into Injury Prevention Practice
ing, officer candidate school, or a service academy. Injury (TRIPP) model.
incidence during these stages of training is extremely high:
Approximately 27% of men and 57% of women will sustain
MSK-Is during this time. Importantly, these figures do not
6–8
account for the additional percentages of people who enter ser-
vice with a history of MSK-I. Although almost 25% of those
with injuries will go on to be separated from service (many of
whom may try again at a later date), most are recycled into
training and continue on to the next training phase. Service-
9
members wishing to become part of a SOF community may
have gone through numerous cycles of training, deployment,
and rest, and be left managing pain and dysfunction from a
previous MSK-I, repeated MSK-I, or a primary MSK-I.
Whether these MSK-Is are primary, secondary, or tertiary is
known only to the Servicemember and, to our knowledge, no
scientific studies have addressed this question. This gap ham- IP, injury prevention; MSK, musculoskeletal; RCT, randomized con-
pers the first two stages of the traditional MSK-I prevention trolled trial.
model in which injury surveillance is conducted and etiol-
ogy and mechanisms of injury are established. Additionally, Integrating MSK-I Prevention Across the
10
many proven MSK-I prevention efforts are complicated by the Training Continuum
inability to effectively implement them. Emerging literature
from the sports world shows that an expanded injury preven- MSK-I prevention approaches in the military can be progres-
tion model (Figure 2) may be necessary for MSK-I prevention sive, targeted, integrated, and effective if set up properly. Over
efforts to be effectively implemented and sustained. 10–14 the past decades, many risk factors for MSK-I in basic train-
ing have been successfully identified, but success in reducing
Without a true understanding of MSK-I at the basic levels MSK-I is limited, in part because few studies have followed
of surveillance and etiology continuously throughout the life Servicemembers over the course of their careers. Although a
cycle, and without sufficient implementation issues factored history of injury before entering training, cardiovascular fit-
15
in to their development, current MSK-I prevention programs ness, muscular strength and endurance, smoking history,
17
15
16
will be challenged to sufficiently reduce MSK within any com- sex, and functional movement patterns 18–21 have served as the
munity, much less the SOF. Thus, the question remains: What basis for many MSK-I prevention initiatives, early attempts
is the best way to prevent MSK-I? We believe expanding on in basic training produced mixed results. Efforts to prescribe
MSK-I prevention efforts in basic training is essential because running shoes on the basis the foot type showed limited ef-
here injury surveillance and etiology have been thoroughly fects on reducing injury, 22,23 and smoking cessation, although
documented for nearly three decades. Although some suc- effective in the long term, can take months to years to reverse
cesses have been shown, these efforts must continue in a coor- the negative effects of smoking. Reducing overall running
24
dinated fashion throughout the life cycle. mileage and dividing basic trainees into run-ability groups
98 | JSOM Volume 17, Edition 4/Winter 2017