
Page 86 - Journal of Special Operations Medicine - Fall 2017
P. 86
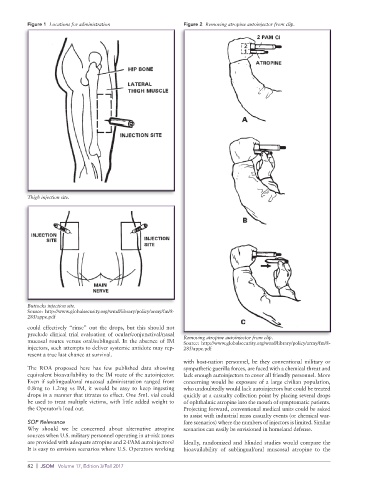
Figure 1 Locations for administration Figure 2 Removing atropine autoinjector from clip.
Thigh injection site.
Buttocks injection site.
Source: http://www.globalsecurity.org/wmd/library/policy/army/fm/8-
285/appe.pdf
could effectively “rinse” out the drops, but this should not
preclude clinical trial evaluation of ocular/conjunctival/nasal
mucosal routes versus oral/sublingual. In the absence of IM Removing atropine autoinjector from clip.
Source: http://www.globalsecurity.org/wmd/library/policy/army/fm/8-
injectors, such attempts to deliver systemic antidote may rep- 285/appe.pdf
resent a true last chance at survival.
with host-nation personnel, be they conventional military or
The ROA proposed here has few published data showing sympathetic guerilla forces, are faced with a chemical threat and
equivalent bioavailability to the IM route of the autoinjector. lack enough autoinjectors to cover all friendly personnel. More
Even if sublingual/oral mucosal administration ranged from concerning would be exposure of a large civilian population,
0.8mg to 1.2mg vs IM, it would be easy to keep ingesting who undoubtedly would lack autoinjectors but could be treated
drops in a manner that titrates to effect. One 5mL vial could quickly at a casualty collection point by placing several drops
be used to treat multiple victims, with little added weight to of ophthalmic atropine into the mouth of symptomatic patients.
the Operator’s load out. Projecting forward, conventional medical units could be asked
to assist with industrial mass casualty events (or chemical war-
SOF Relevance fare scenarios) where the numbers of injectors is limited. Similar
Why should we be concerned about alternative atropine scenarios can easily be envisioned in homeland defense.
sources when U.S. military personnel operating in at-risk zones
are provided with adequate atropine and 2-PAM autoinjectors? Ideally, randomized and blinded studies would compare the
It is easy to envision scenarios where U.S. Operators working bioavailability of sublingual/oral muscosal atropine to the
82 | JSOM Volume 17, Edition 3/Fall 2017