
Page 81 - Journal of Special Operations Medicine - Fall 2014
P. 81
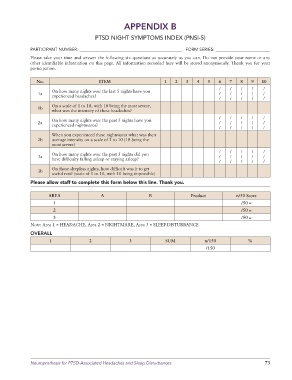
APPENDIX B
PTSD NIGHT SYMPTOMS INDEX (PNSI-5)
PARTICIPANT NUMBER: _______________________________________________ FORM SERIES: _________________________
Please take your time and answer the following six questions as accurately as you can. Do not provide your name or any
other identifiable information on this page. All information recorded here will be stored anonymously. Thank you for your
participation.
No. ITEM 1 2 3 4 5 6 7 8 9 10
/ / / / /
On how many nights over the last 5 nights have you
1a / / / / /
experienced headaches?
/ / / / /
On a scale of 1 to 10, with 10 being the most severe,
1b
what was the intensity of these headaches?
/ / / / /
On how many nights over the past 5 nights have you
2a / / / / /
experienced nightmares?
/ / / / /
When you experienced these nightmares what was their
2b average intensity on a scale of 1 to 10 (10 being the
most severe)
/ / / / /
On how many nights over the past 5 nights did you
3a / / / / /
have difficulty falling asleep or staying asleep?
/ / / / /
On those sleepless nights, how difficult was it to get
3b
useful rest? (scale of 1 to 10, with 10 being impossible)
Please allow staff to complete this form below this line. Thank you.
AREA A B Product n/50 Score
1 /50 =
2 /50 =
3 /50 =
Note: Area 1 = HEADACHE, Area 2 = NIGHTMARE, Area 3 = SLEEP DISTURBANCE
OVERALL
1 2 3 SUM n/150 %
/150
Neuroprothesis for PTSD-Associated Headaches and Sleep Disturbances 73