
Page 107 - Journal of Special Operations Medicine - Spring 2014
P. 107
An Ongoing Series
Giant Basal Cell Carcinoma
Shayna C. Rivard, MD; Michael L. Crandall, MD; Neil F. Gibbs, MD
ABSTRACT
Servicemembers are often exposed to extreme environments Case Report
with sun exposure, often laying the foundation for future A 36-year-old male active duty Seabee presents to your
skin cancer. Basal cell carcinoma (BCC) is the most com- office with a left shoulder plaque that initially started
mon of skin cancers. We present the case of a 36-year-old as an erythematous papule but has now increased to
male active duty Seabee who presents with a left shoulder greater than 6cm in the past 10 years. He has no signifi-
plaque that initially started as an erythematous papule but cant past medical history. He reports that it occasionally
has now increased to greater than 6cm in the past 10 years itches and burns but is overall not bothersome. He notes
and is diagnosed as giant basal cell carcinoma (GBCC). Al- no known inciting event and has no other symptoms.
though only 0.5% to 1% of BCCs develop into GBCCs, there His job occupation includes spending a lot of time in
is the potential for metastasis and even death. This article bright sunlight. The patient reports no other history of
addresses the concerning and potentially fatal diagnosis of prior skin disorders.
GBCC, including your initial impressions and differential di-
agnoses, available treatment options, and ways to prevent it On examination, he has one large erythematous plaque
from ever occurring in our military population.
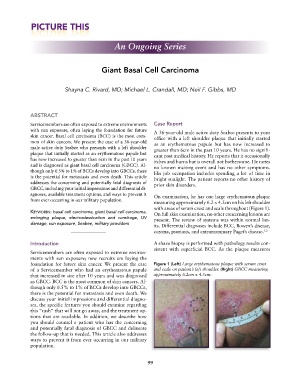
measuring approximately 6.2 × 4.5cm on his left shoulder
with areas of serum crust and scale throughout (Figure 1).
Keywords: basal cell carcinoma, giant basal cell carcinoma, On full skin examination, no other concerning lesions are
enlarging plaque, electrodessication and curettage, UV present. The review of systems was within normal lim-
damage, sun exposure, Seabee, military providers
its. Differential diagnoses include BCC, Bowen’s disease,
eczema, psoriasis, and extramammary Paget’s disease. 1,2
Introduction A shave biopsy is performed with pathology results con-
sistent with superficial BCC. As the plaque measures
Servicemembers are often exposed to extreme environ-
ments with sun exposure; new recruits are laying the
foundation for future skin cancer. We present the case Figure 1 (Left) Large erythematous plaque with serum crust
of a Servicemember who had an erythematous papule and scale on patient’s left shoulder. (Right) GBCC measuring
that increased in size after 10 years and was diagnosed approximately 6.2cm × 4.5cm.
as GBCC. BCC is the most common of skin cancers. Al-
though only 0.5% to 1% of BCCs develop into GBCCs,
there is the potential for metastasis and even death. We
discuss your initial impressions and differential diagno-
ses, the specific features you should examine regarding
this “rash” that will not go away, and the treatment op-
tions that are available. In addition, we describe how
you should counsel a patient who has the concerning
and potentially fatal diagnosis of GBCC and delineate
the follow-up that is needed. This article also addresses
ways to prevent it from ever occurring in our military
population.
99