
Page 10 - Journal of Special Operations Medicine - Spring 2014
P. 10
On arrival at the Role 2 facility, he was unconscious Figure 2 Case 1: The escharotomy was packed with saline-
with spontaneous breathing and a Glasgow Coma Scale moistened Kerlix bandages.
score of less than 8. He sustained neurological decline
during the helicopter evacuation. He did not present
with any fractures or internal organ lesions.
Immediate Advanced Trauma Life Support (ATLS) proto-
cols were applied. The patient was intubated with some
difficulty due to the presence of edema in the airway. At
first, it was impossible to obtain venous access, so we es-
tablished intraosseous access at the tibia. This was later
replaced by a central venous catheter in the right sub-
clavian vein once in the operating room. We initiated
fluid resuscitation according to the Parkland formula and
started intraosseous antibiotic therapy. In the operating
room, the surgeons performed an escharotomy of the
upper limbs (Figure 1) and debridement of necrotic blis-
ters. They packed the escharotomy with saline-moistened
™
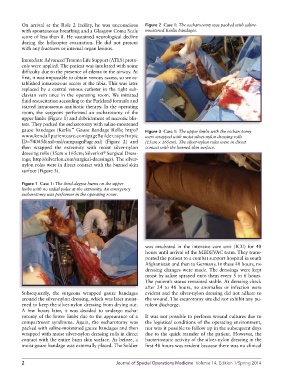
gauze bandages (Kerlix Gauze Bandage Rolls; http:// Figure 3 Case 1: The upper limbs with the escharotomy
www.kendallpatientcare.com/pageBuilder.aspx?topic were wrapped with moist silver-nylon dressing rolls
ID=74045&xsl=xsl/campaignPage.xsl) (Figure 2) and (15cm × 165cm). The silver-nylon roles were in direct
then wrapped the extremity with moist silver-nylon contact with the burned skin surface.
®
dressing rolls (15cm × 165cm; Silverlon Surgical Dress-
ings; http://silverlon.com/surgical-dress ings). The silver-
nylon roles were in direct contact with the burned skin
surface (Figure 3).
Figure 1 Case 1: The third-degree burns on the upper
limbs with no radial pulse at the extremity. An emergency
escharotomy was performer in the operating room.
was intubated in the intensive care unit (ICU) for 48
hours until arrival of the MEDEVAC team. They trans-
ported the patient to a combat support hospital in south
Afghanistan and then to Germany. In these 48 hours, no
dressing changes were made. The dressings were kept
moist by saline sprayed onto them every 5 to 6 hours.
The patient’s status remained stable. At dressing check
after 24 to 48 hours, no anomalies or infection were
Subsequently, the surgeons wrapped gauze bandages evident and the silver-nylon dressing did not adhere to
around the silver-nylon dressing, which was later moist- the wound. The escarotomy site did not exhibit any pu-
ened to keep the silver-nylon dressing from drying out. rulent discharge.
A few hours later, it was decided to undergo escha-
rotomy of the lower limbs due to the appearance of a It was not possible to perform wound cultures due to
compartment syndrome. Again, the escharotomy was the logistical conditions of the operating environment,
packed with saline-moistened gauze bandages and then nor was it possible to follow up in the subsequent days
wrapped with moist silver-nylon dressing rolls in direct due to the quick transfer of the patient. However, the
contact with the entire burn skin surface. As before, a bacteriostatic activity of the silver-nylon dressing in the
moist gauze bandage was externally placed. The Soldier first 48 hours was evident because there was no clinical
2 Journal of Special Operations Medicine Volume 14, Edition 1/Spring 2014