
Page 377 - ATP-P 11th Ed
P. 377
Surgical Airways
a. Surgical airways are not warranted in an unconscious or anesthetized MWD that has
no direct upper airway trauma unless the performance of basic airway positioning
maneuvers is unsuccessful in opening the airway and/or the provider is unable to
successfully perform ETI.
b. Surgical Cricothyrotomy (CTT)
i. Use techniques recommended for humans.
(a) Bougie-aided open surgical, flanged and cuffed airway cannula, 6–9mm in-
ternal diameter, 5–8cm intratracheal length.
(b) Standard open surgical, flanged and cuffed airway cannula, 6 – 9mm inter-
nal diameter, 5–8cm intratracheal length.
c. Surgical Tube Tracheostomy (TT)
i. Use the largest internal diameter tube that fits into the MWD’s trachea; aim for a
TT that is at least 70% of the estimated internal tracheal lumen diameter.
ii. Select a TT length of 5–8cm or one that does not extend beyond the thoracic
inlet/point of shoulder.
iii. Blind Insertion Airway Device/Nasopharyngeal Airways/Extraglottic Airway
Devices have not been evaluated in canines and should not be utilized in MWDs. SECTION 4
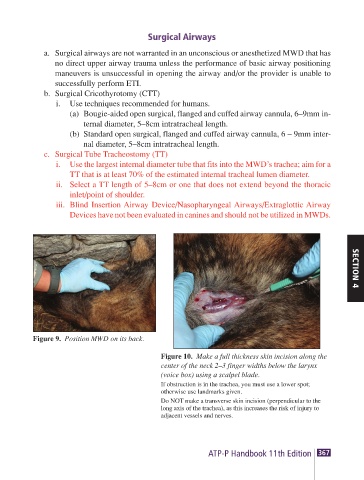
Figure 9. Position MWD on its back.
Figure 10. Make a full thickness skin incision along the
center of the neck 2–3 finger widths below the larynx
(voice box) using a scalpel blade.
If obstruction is in the trachea, you must use a lower spot;
otherwise use landmarks given.
Do NOT make a transverse skin incision (perpendicular to the
long axis of the trachea), as this increases the risk of injury to
adjacent vessels and nerves.
ATP-P Handbook 11th Edition 367