
Page 221 - 2023 SMOG Digital
P. 221
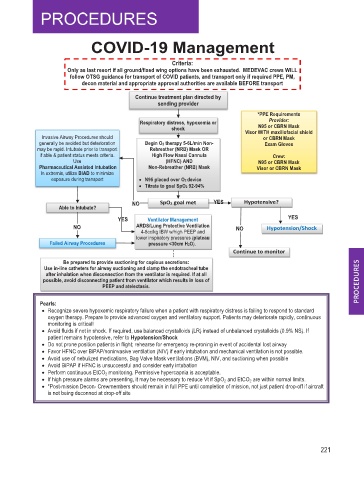
COVID-19 Management
Criteria:
Only as last resort if all ground/fixed wing options have been exhausted. MEDEVAC crews WILL
follow OTSG guidance for transport of COVID patients, and transport only if required PPE, PM,
decon material and appropriate approval authorities are available BEFORE transport
Continue treatment plan directed by
sending provider
*PPE Requirements
Respiratory distress, hypoxemia or Provider:
N95 or CBRN Mask
shock Visor WITH maxillofacial shield
Invasive Airway Procedures should or CBRN Mask
generally be avoided but deterioration Begin O2 therapy 5-6L/min Non- Exam Gloves
may be rapid. Intubate prior to transport Rebreather (NRB) Mask OR
if able & patient status meets criteria. High Flow Nasal Cannula Crew:
Use (HFNC) AND N95 or CBRN Mask
Pharmaceutical Assisted Intubation Non-Rebreather (NRB) Mask Visor or CBRN Mask
In extremis, utilize BIAD to minimize
exposure during transport • N95 placed over O2 device
• Titrate to goal SpO2 92-94%
NO SpO2 goal met YES Hypotensive?
Able to Intubate?
YES Ventilator Management YES
NO ARDS/Lung Protective Ventilation NO Hypotension/Shock
4-8cc/kg IBW w/high PEEP and
lower inspiratory pressures (plateau
Failed Airway Procedures pressure <30cm H2O).
Continue to monitor
Be prepared to provide suctioning for copious secretions:
Use in-line catheters for airway suctioning and clamp the endotracheal tube
after inhalation when disconnection from the ventilator is required. If at all
possible, avoid disconnecting patient from ventilator which results in loss of
PEEP and atelectasis.
Pearls:
• Recognize severe hypoxemic respiratory failure when a patient with respiratory distress is failing to respond to standard
oxygen therapy. Prepare to provide advanced oxygen and ventilatory support. Patients may deteriorate rapidly, continuous
monitoring is critical!
• Avoid fluids if not in shock. If required, use balanced crystalloids (LR) instead of unbalanced crystalloids (0.9% NS). If
patient remains hypotensive, refer to Hypotension/Shock
• Do not prone position patients in flight; rehearse for emergency re-proning in event of accidental lost airway
• Favor HFNC over BiPAP/noninvasive ventilation (NIV) if early intubation and mechanical ventilation is not possible.
• Avoid use of nebulized medications, Bag Valve Mask ventilations (BVM), NIV, and suctioning when possible
• Avoid BiPAP if HFNC is unsuccessful and consider early intubation
• Perform continuous EtCO 2 monitoring. Permissive hypercapnia is acceptable.
• If high pressure alarms are presenting, it may be necessary to reduce Vt if SpO 2 and EtCO 2 are within normal limits.
• *Post-mission Decon- Crewmembers should remain in full PPE until completion of mission, not just patient drop-off if aircraft
is not being deconned at drop-off site
221