
Page 258 - PJ MED OPS Handbook 8th Ed
P. 258
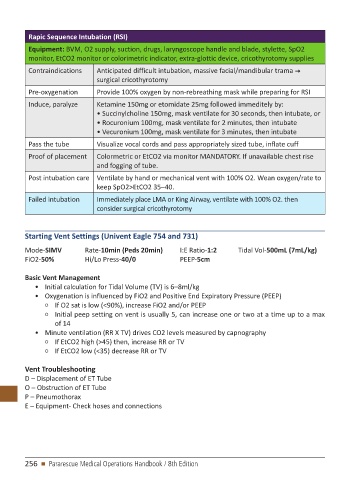
Rapic Sequence Intubation (RSI)
Equipment: BVM, O2 supply, suction, drugs, laryngoscope handle and blade, stylette, SpO2
monitor, EtCO2 monitor or colorimetric indicator, extra-glottic device, cricothyrotomy supplies
Contraindications Anticipated difficult intubation, massive facial/mandibular trama
surgical cricothyrotomy
Pre-oxygenation Provide 100% oxygen by non-rebreathing mask while preparing for RSI
Induce, paralyze Ketamine 150mg or etomidate 25mg followed immeditely by:
• Succinylcholine 150mg, mask ventilate for 30 seconds, then intubate, or
• Rocuronium 100mg, mask ventilate for 2 minutes, then intubate
• Vecuronium 100mg, mask ventilate for 3 minutes, then intubate
Pass the tube Visualize vocal cords and pass appropriately sized tube, inflate cuff
Proof of placement Colormetric or EtCO2 via monitor MANDATORY. If unavailable chest rise
and fogging of tube.
Post intubation care Ventilate by hand or mechanical vent with 100% O2. Wean oxygen/rate to
keep SpO2>EtCO2 35–40.
Failed intubation Immediately place LMA or King Airway, ventilate with 100% O2. then
consider surgical cricothyrotomy
Starting Vent Settings (Univent Eagle 754 and 731)
Mode-SIMV Rate-10min (Peds 20min) I:E Ratio-1:2 Tidal Vol-500mL (7mL/kg)
FiO2-50% Hi/Lo Press-40/0 PEEP-5cm
Basic Vent Management
• Initial calculation for Tidal Volume (TV) is 6–8ml/kg
• Oxygenation is influenced by FiO2 and Positive End Expiratory Pressure (PEEP)
○ If O2 sat is low (<90%), increase FiO2 and/or PEEP
○ Initial peep setting on vent is usually 5, can increase one or two at a time up to a max
of 14
• Minute ventilation (RR X TV) drives CO2 levels measured by capnography
○ If EtCO2 high (>45) then, increase RR or TV
○ If EtCO2 low (<35) decrease RR or TV
Vent Troubleshooting
D – Displacement of ET Tube
O – Obstruction of ET Tube
P – Pneumothorax
E – Equipment- Check hoses and connections
256 n Pararescue Medical Operations Handbook / 8th Edition