
Page 27 - JSOM Winter 2024
P. 27
difference of 60 seconds between techniques for FWB collec- TABLE 1 Volunteer Demographics
tion times. This represents approximately 10% of the upper PIV access technique
limit for FWB collection times described by the American Red Total, no. (%); performed first, no. (%)
Cross as well as prior medic-based IV literature. 11,12 Using a n=23 SLT; n=10 SST; n=13
crossover design, a power analysis established a required sam- Sex
ple size of 15 medics to complete both arms of the study.
Male 21 (92) 8 (80) 13 (100)
Continuous variables, including time, rate accuracy, volume ac- Female 1 (4) 1 (10) 0 (0)
curacy, and user confidence, were analyzed using a Mann-Whit- Preferred no answer 1 (4) 1 (10) 0 (0)
ney U test, while ordinal data of user appraisal was analyzed Age, yr 5 (50) 7 (54)
using a Wilcoxon Signed-Rank test. Demographic data was 18–22 12 (52) 4 (40) 5 (38)
evaluated using Microsoft Excel (Microsoft Corp., Seattle, 23–30 9 (39) 1 (10) 1 (8)
WA), while all other data was analyzed with DATAtab: Online >31 2 (9)
Statistics Calculator (DATAtab e.U., Graz, Austria).
Grade
E2–E3 8 (35) 3 (30) 5 (39)
Results E4 11 (48) 5 (50) 6 (46)
A total of 72 U.S. Army medics initially volunteered for study E5-E6 4 (17) 2 (20) 2 (15)
participation, with 24 selected to perform venipuncture by ran- Time in service, mo
domization. One volunteer selected to perform venipuncture <12 4 (17) 0 (0) 4 (31)
withdrew from study participation citing lack of comfort while 12–24 8 (35) 5 (50) 3 (23)
performing the procedure. The remaining 23 medics completed 25–48 6 (26) 3 (30) 3 (23)
a total of 46 FWB collections over 6 days of testing. The median >48 5 (22) 2 (20) 3 (23)
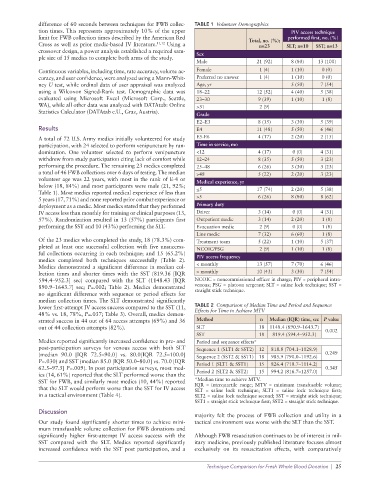
volunteer age was 22 years, with most in the rank of E-4 or Medical experience, yr
below (18, 84%) and most participants were male (21, 92%;
Table 1). Most medics reported medical experience of less than <5 17 (74) 2 (20) 5 (38)
5 years (17, 71%) and none reported prior combat experience or >5 6 (26) 8 (80) 8 (62)
deployment as a medic. Most medics stated that they performed Primary duty
IV access less than monthly for training or clinical purposes (13, Driver 3 (14) 0 (0) 4 (31)
57%). Randomization resulted in 13 (57%) participants first Outpatient medic 3 (14) 2 (20) 1 (8)
performing the SST and 10 (43%) performing the SLT. Evacuation medic 2 (9) 0 (0) 1 (8)
Line medic 7 (32) 6 (60) 1 (8)
Of the 23 medics who completed the study, 18 (78.3%) com- Treatment team 5 (22) 1 (10) 5 (37)
pleted at least one successful collection with five unsuccess- NCOIC/PSG 2 (9) 1 (10) 1 (8)
ful collections occurring in each technique; and 15 (65.2%)
medics completed both techniques successfully (Table 2). PIV access frequency
Medics demonstrated a significant difference in median col- < monthly 13 (57) 7 (70) 6 (46)
lection times and shorter times with the SST (819.36 [IQR > monthly 10 (43) 3 (30) 7 (54)
594.4–952.3] sec) compared with the SLT (1148.43 [IQR NCOIC = noncommissioned officer in charge; PIV = peripheral intra-
890.9–1643.7] sec; P=.002; Table 2). Medics demonstrated venous; PSG = platoon sergeant; SLT = saline lock technique; SST =
no significant difference with sequence or period effects for straight stick technique.
median collection times. The SLT demonstrated significantly
lower first-attempt IV access success compared to the SST (11, TABLE 2 Comparison of Median Time and Period and Sequence
48% vs. 18, 78%, P=.037; Table 3). Overall, medics demon- Effects for Time to Achieve MTV
strated success in 44 out of 64 access attempts (69%) and 36 Method n Median (IQR) time, sec P value
out of 44 collection attempts (82%). SLT 18 1148.4 (890.9–1643.7) 0.002
SST 18 819.4 (594.4–952.3)
Medics reported significantly increased confidence in pre- and Period and sequence effects*
post-participation surveys for venous access with both SLT Sequence 1 (SLT1 & SST2) 12 818.8 (704.1–1028.9)
(median 90.0 [IQR 72.5–90.0] vs. 80.0[IQR 72.5–100.0] Sequence 2 (SST2 & SST1) 18 985.9 (790.0–1192.6) 0.249
P=.030) and SST (median 85.0 [IQR 50.0–80.0] vs. 70.0 [IQR Period 1 (SLT1 & SST1) 15 826.4 (718.7–1114.2)
62.5–97.5] P=.009). In post participation surveys, most med- 0.345
ics (14, 61%) reported that the SLT performed worse than the Period 2 (SLT2 & SST2) 15 994.2 (816.7–1257.0)
SST for FWB, and similarly most medics (10, 44%) reported *Median time to achieve MTV.
that the SLT would perform worse than the SST for IV access IQR = interquartile range; MTV = minimum transfusable volume;
SLT = saline lock technique; SLT1 = saline lock technique first;
in a tactical environment (Table 4). SLT2 = saline lock technique second; SST = straight stick technique;
SST1 = straight stick technique first; SST2 = straight stick technique.
Discussion
majority felt the process of FWB collection and utility in a
Our study found significantly shorter times to achieve mini- tactical environment was worse with the SLT than the SST.
mum transfusable volume collection for FWB donations and
significantly higher first-attempt IV access success with the Although FWB resuscitation continues to be of interest in mil-
SST compared with the SLT. Medics reported significantly itary medicine, previously published literature focuses almost
increased confidence with the SST post participation, and a exclusively on its resuscitation effects, with comparatively
Technique Comparison for Fresh Whole Blood Donation | 25