
Page 14 - JSOM Summer 2024
P. 14
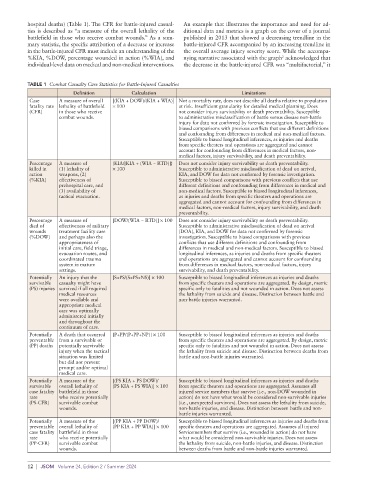
hospital deaths) (Table 1). The CFR for battle-injured casual- An example that illustrates the importance and need for ad-
ties is described as “a measure of the overall lethality of the ditional data and metrics is a graph on the cover of a journal
battlefield in those who receive combat wounds.” As a sum- published in 2013 that showed a decreasing trendline in the
mary statistic, the specific attribution of a decrease or increase battle-injured CFR accompanied by an increasing trendline in
in the battle-injured CFR must include an understanding of the the overall average injury severity score. While the accompa-
2
%KIA, %DOW, percentage wounded in action (%WIA), and nying narrative associated with the graph acknowledged that
individual-level data on medical and non-medical interventions. the decrease in the battle-injured CFR was “multifactorial,” it
TABLE 1 Combat Casualty Care Statistics for Battle-Injured Casualties
Definition Calculation Limitations
Case A measure of overall [(KIA + DOW)/(KIA + WIA)] Not a mortality rate, does not describe all deaths relative to population
fatality rate lethality of battlefield × 100 at risk. Insufficient granularity for detailed medical planning. Does
(CFR) in those who receive not consider injury survivability or death preventability. Susceptible
combat wounds. to administrative misclassification of battle versus disease non-battle
injury for data not confirmed by forensic investigation. Susceptible to
biased comparisons with previous conflicts that use different definitions
and confounding from differences in medical and non-medical factors.
Susceptible to biased longitudinal inferences, as injuries and deaths
from specific theaters and operations are aggregated and cannot
account for confounding from differences in medical factors, non-
medical factors, injury survivability, and death preventability.
Percentage A measure of {KIA/[KIA + (WIA − RTD)]} Does not consider injury survivability or death preventability.
killed in (1) lethality of × 100 Susceptible to administrative misclassification of dead on arrival,
action weapons, (2) KIA, and DOW for data not confirmed by forensic investigation.
(%KIA) effectiveness of Susceptible to biased comparisons with previous conflicts that use
prehospital care, and different definitions and confounding from differences in medical and
(3) availability of non-medical factors. Susceptible to biased longitudinal inferences,
tactical evacuation. as injuries and deaths from specific theaters and operations are
aggregated and cannot account for confounding from differences in
medical factors, non-medical factors, injury survivability, and death
preventability.
Percentage A measure of [DOW/(WIA − RTD)] × 100 Does not consider injury survivability or death preventability.
died of effectiveness of military Susceptible to administrative misclassification of dead on arrival
wounds treatment facility care (DOA), KIA, and DOW for data not confirmed by forensic
(%DOW) and perhaps also the investigation. Susceptible to biased comparisons with previous
appropriateness of conflicts that use different definitions and confounding from
initial care, field triage, differences in medical and non-medical factors. Susceptible to biased
evacuation routes, and longitudinal inferences, as injuries and deaths from specific theaters
coordinated trauma and operations are aggregated and cannot account for confounding
system in mature from differences in medical factors, non-medical factors, injury
settings. survivability, and death preventability.
Potentially An injury that the [S+PS/(S+PS+NS)] × 100 Susceptible to biased longitudinal inferences as injuries and deaths
survivable casualty might have from specific theaters and operations are aggregated. By design, metric
(PS) injuries survived if all required specific only to fatalities and not wounded in action. Does not assess
medical resources the lethality from suicide and disease. Distinction between battle and
were available and non-battle injuries warranted.
appropriate medical
care was optimally
administered initially
and throughout the
continuum of care.
Potentially A death that occurred [P+PP/(P+PP+NP)] × 100 Susceptible to biased longitudinal inferences as injuries and deaths
preventable from a survivable or from specific theaters and operations are aggregated. By design, metric
(PP) deaths potentially survivable specific only to fatalities and not wounded in action. Does not assess
injury when the tactical the lethality from suicide and disease. Distinction between deaths from
situation was limited battle and non-battle injuries warranted.
but did not prevent
prompt and/or optimal
medical care.
Potentially A measure of the [(PS KIA + PS DOW)/ Susceptible to biased longitudinal inferences as injuries and deaths
survivable overall lethality of (PS KIA + PS WIA)] × 100 from specific theaters and operations are aggregated. Assumes all
case fatality battlefield in those injured service members that survive (i.e., non-DOW wounded in
rate who receive potentially action) do not have what would be considered non-survivable injuries
(PS-CFR) survivable combat (i.e., unexpected survivors). Does not assess the lethality from suicide,
wounds. non-battle injuries, and disease. Distinction between battle and non-
battle injuries warranted.
Potentially A measure of the [(PP KIA + PP DOW)/ Susceptible to biased longitudinal inferences as injuries and deaths from
preventable overall lethality of (PP KIA + PP WIA)] × 100 specific theaters and operations are aggregated. Assumes all injured
case fatality battlefield in those Servicemembers that survive (i.e., wounded in action) do not have
rate who receive potentially what would be considered non-survivable injuries. Does not assess
(PP-CFR) survivable combat the lethality from suicide, non-battle injuries, and disease. Distinction
wounds. between deaths from battle and non-battle injuries warranted.
12 | JSOM Volume 24, Edition 2 / Summer 2024