
Page 76 - JSOM Summer 2023
P. 76
accessible means of REBOA placement confirmation is neces- fluoroscopy and marking both on the catheter itself and re-
sary. This study evaluated the accuracy and reliability of US in cording the depth inserted in centimeters. For Zone 1, the
the localization of REBOA catheter placement in Zones 1 and REBOA balloon was inflated with 8mL of normal saline, and
3 of the aorta in a pressurized cadaver model. for Zone 3, it was inflated with 2mL of normal saline.
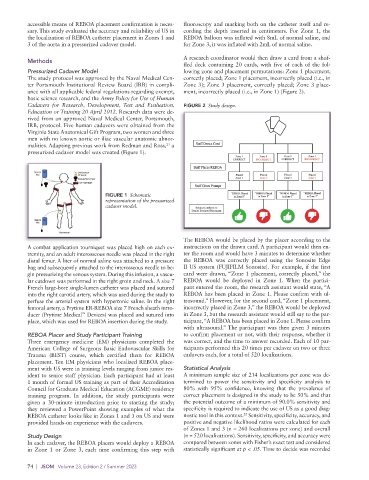
A research coordinator would then draw a card from a shuf-
Methods
fled deck containing 20 cards, with five of each of the fol-
Pressurized Cadaver Model lowing zone and placement permutations: Zone 1 placement,
The study protocol was approved by the Naval Medical Cen- correctly placed; Zone 1 placement, incorrectly placed (i.e., in
ter Portsmouth Institutional Review Board (IRB) in compli- Zone 3); Zone 3 placement, correctly placed; Zone 3 place-
ance with all applicable federal regulations regarding exempt, ment, incorrectly placed (i.e., in Zone 1) (Figure 2).
basic science research, and the Army Policy for Use of Human
Cadavers for Research, Development, Test and Evaluation, FIGURE 2 Study design.
Education or Training 20 April 2012. Research data were de-
rived from an approved Naval Medical Center, Portsmouth,
IRB, protocol. Five human cadavers were obtained from the
Virginia State Anatomical Gift Program, two women and three
men with no known aortic or iliac vascular anatomic abnor-
malities. Adapting previous work from Redman and Ross, a
21
pressurized cadaver model was created (Figure 1).
FIGURE 1 Schematic
representation of the pressurized
cadaver model.
The REBOA would be placed by the placer according to the
A combat application tourniquet was placed high on each ex- instructions on the drawn card. A participant would then en-
tremity, and an adult interosseous needle was placed in the right ter the room and would have 3 minutes to determine whether
distal femur. A liter of normal saline was attached to a pressure the REBOA was correctly placed using the Sonosite Edge
bag and subsequently attached to the interosseous needle to be- II US system (FUJIFILM Sonosite). For example, if the first
gin pressurizing the venous system. During this infusion, a vascu- card were drawn, “Zone 1 placement, correctly placed,” the
lar cutdown was performed in the right groin and neck. A size 7 REBOA would be deployed in Zone 1. When the partici-
French large-bore single-lumen catheter was placed and sutured pant entered the room, the research assistant would state, “A
into the right carotid artery, which was used during the study to REBOA has been placed in Zone 1. Please confirm with ul-
perfuse the arterial system with hypertonic saline. In the right trasound.” However, for the second card, “Zone 1 placement,
femoral artery, a Prytime ER-REBOA size 7 French sheath intro- incorrectly placed in Zone 3,” the REBOA would be deployed
™
ducer (Prytime Medical Devices) was placed and sutured into in Zone 3, but the research assistant would still say to the par-
place, which was used for REBOA insertion during the study. ticipant, “A REBOA has been placed in Zone 1. Please confirm
with ultrasound.” The participant was then given 3 minutes
REBOA Placer and Study Participant Training to confirm placement or not, with their response, whether it
Three emergency medicine (EM) physicians completed the was correct, and the time to answer recorded. Each of 10 par-
American College of Surgeons Basic Endovascular Skills for ticipants performed this 20 times per cadaver on two or three
Trauma (BEST) course, which certified them for REBOA cadavers each, for a total of 520 localizations.
placement. Ten EM physicians who localized REBOA place-
ment with US were in training levels ranging from junior res- Statistical Analysis
ident to senior staff physician. Each participant had at least A minimum sample size of 214 localizations per zone was de-
1 month of formal US training as part of their Accreditation termined to power the sensitivity and specificity analysis to
Council for Graduate Medical Education (ACGME) residency 80% with 95% confidence, knowing that the prevalence of
training program. In addition, the study participants were correct placement is designed in the study to be 50% and that
given a 30-minute introduction prior to starting the study; the potential outcome of a minimum of 90.0% sensitivity and
they reviewed a PowerPoint showing examples of what the specificity is required to indicate the use of US as a good diag-
22
REBOA catheter looks like in Zones 1 and 3 on US and were nostic tool in this context. Sensitivity, specificity, accuracy, and
provided hands-on experience with the cadavers. positive and negative likelihood ratios were calculated for each
of Zones 1 and 3 (n = 260 localizations per zone) and overall
Study Design (n = 520 localizations). Sensitivity, specificity, and accuracy were
In each cadaver, the REBOA placers would deploy a REBOA compared between zones with Fisher’s exact test and considered
in Zone 1 or Zone 3, each time confirming this step with statistically significant at p < .05. Time to decide was recorded
74 | JSOM Volume 23, Edition 2 / Summer 2023