
Page 53 - JSOM Summer 2023
P. 53
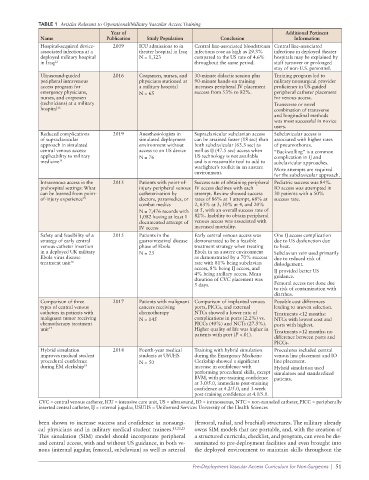
TABLE 1 Articles Relevant to Operational/Military Vascular Access Training
Year of Additional Pertinent
Name Publication Study Population Conclusion Information
Hospital-acquired device- 2009 ICU admissions to in Central line-associated bloodstream Central line-associated
associated infections at a theater hospital in Iraq infections rose as high as 29.3% infections in deployed theater
deployed military hospital N = 1,323 compared to the US rate of 4.6% hospitals may be explained by
in Iraq 12 throughout the same period. staff turnover or prolonged
stay of non-U.S. personnel.
Ultrasound-guided 2016 Corpsmen, nurses, and 30-minute didactic session plus Training program led to
peripheral intravenous physicians stationed at 90-minute hands-on training military nonsurgical provider
access program for a military hospital increases peripheral IV placement proficiency in US-guided
emergency physicians, N = 65 success from 53% to 82%. peripheral catheter placement
nurses, and corpsmen for venous access.
(technicians) at a military Transverse or novel
hospital 13 combination of transverse
and longitudinal methods
was most successful in novice
users.
Reduced complications 2019 Anesthesiologists in Supraclavicular subclavian access Subclavicular access is
of supraclavicular simulated deployment can be attained faster (18 sec) than associated with higher rates
approach in simulated environment without both subclavicular (63.3 sec) as of pneumothorax.
central venous access: access to an US device well as IJ (47.5 sec) access when “Backwalling” is a common
applicability to military N = 76 US technology is not available complication in IJ and
medicine 14 and is a reasonable tool to add to subclavicular approaches.
warfighter’s toolkit in an austere More attempts are required
environment.
for the subclavicular approach.
Intravenous access in the 2015 Patients with point-of- Success rate of obtaining peripheral Pediatric success was 84%.
prehospital settings: What injury peripheral venous IV access declines with each IO access was attempted in
can be learned from point- catheterization by attempt. Review showed success 30 patients with a 50%
of-injury experience 15 doctors, paramedics, or rates of 86% at 1 attempt, 68% at success rate.
combat medics 2, 63% at 3, 50% at 4, and 20%
N = 7,476 records with at 5, with an overall success rate of
1,082 having at least 1 82%. Inability to obtain peripheral
documented attempt of venous access was associated with
IV access increased mortality.
Safety and feasibility of a 2015 Patients in the Early central venous access was One IJ access complication
strategy of early central gastrointestinal disease demonstrated to be a feasible due to US dysfunction due
venous catheter insertion phase of Ebola treatment strategy when treating to heat.
in a deployed UK military N = 23 Ebola in an austere environment Subclavian vein used primarily
Ebola virus disease as demonstrated by a 70% success due to reduced risk of
treatment unit 16 rate with 81% being subclavian dislodgement.
access, 8% being IJ access, and IJ provided better US
4% being axillary access. Mean guidance.
duration of CVC placement was
5 days. Femoral access not done due
to risk of contamination with
diarrhea.
Comparison of three 2017 Patients with malignant Comparison of implanted venous Possible cost differences
types of central venous cancers receiving ports, PICCs, and external leading to uneven selection.
catheters in patients with chemotherapy NTCs showed a lower rate of Treatments <12 months:
malignant tumor receiving N = 145 complications in ports (2.2%) vs. NTCs with lowest cost and
chemotherapy treatment PICCs (40%) and NCTs (27.5%). ports with highest.
unit 17 Higher quality of life was higher in Treatments >12 months: no
patients with port (P <.01).
difference between ports and
PICCs.
Hybrid simulation 2014 Fourth-year medical Training with hybrid simulation Procedures included central
improves medical student students at USUHS during the Emergency Medicine venous line placement and IO
procedural confidence N = 50 Clerkship showed a significant line placement.
during EM clerkship 18 increase in confidence with Hybrid simulation used
performing procedural skills, except simulators and standardized
BVM, with pre-training confidence patients.
at 3.0/5.0, immediate post-training
confidence at 4.2/5.0, and 3-week
post-training confidence at 4.1/5.0.
CVC = central venous catheter, ICU = intensive care unit, US = ultrasound, IO = intraosseous, NTC = non-tunneled catheter, PICC = peripherally
inserted central catheter, IJ = internal jugular, USUHS = Uniformed Services University of the Health Sciences
been shown to increase success and confidence in nonsurgi- (femoral, radial, and brachial) structures. The military already
cal physicians and in military medical student trainees. 15,22,23 owns SIM models that are portable, and, with the creation of
This simulation (SIM) model should incorporate peripheral a structured curricula, checklist, and program, can even be dis-
and central access, with and without US guidance, in both ve- seminated to pre-deployment facilities and even brought into
nous (internal jugular, femoral, subclavian) as well as arterial the deployed environment to maintain skills throughout the
Pre-Deployment Vascular Access Curriculum for Non-Surgeons | 51