
Page 50 - JSOM Spring 2023
P. 50
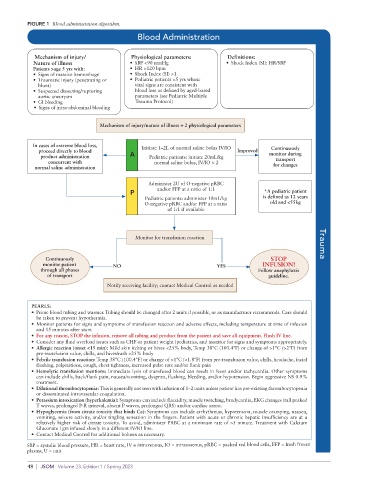
FIGURE 1 Blood administration algorithm.
Blood Administration
Mechanism of injury/ Physiological parameters: Definitions:
Nature of illness • SBP <90 mmHg • Shock Index (SI): HR/SBP
Patients >age 5 yrs with: • HR >120 bpm
• Signs of massive hemorrhage • Shock Index (SI) >1
• Traumatic injury (penetrating or • Pediatric patients >5 yrs whose
blunt) vital signs are consistent with
• Suspected dissecting/rupturing blood loss as defined by aged-based
aortic aneurysm parameters (see Pediatric Multiple
• GI bleeding Trauma Protocol)
• Signs of intra-abdominal bleeding
Mechanism of injury/nature of illness + 2 physiological parameters
In cases of extreme blood loss, Initiate 1–2L of normal saline bolus IV/IO
proceed directly to blood Improved Continuously
product administration A Pediatric patients: initiate 20mL/kg monitor during
concurrent with normal saline bolus, IV/IO × 2 transport
normal saline administration for changes
Administer 2U of O-negative pRBC
P and/or FFP at a ratio of 1:1 *A pediatric patient
Pediatric patients: administer 10mL/kg is defined as 12 years
O-negative pRBC and/or FFP at a ratio old and <55kg
of 1:1 if available
Monitor for transfusion reaction Trauma
Continuously STOP
monitor patient NO YES INFUSION!
through all phases Follow anaphylaxis
of transport guideline.
Notify receiving facility; contact Medical Control as needed
PEARLS:
• Prime blood tubing and warmer. Tubing should be changed after 2 units if possible, or as manufacturer recommends. Care should
be taken to prevent hypothermia.
• Monitor patients for signs and symptoms of transfusion reaction and adverse effects, including temperature at time of infusion
and 15 minutes after start.
• For any reason, STOP the infusion, remove all tubing and product from the patient and save all equipment. Flush IV line.
• Consider any fluid overload issues such as CHF or patient weight (pediatrics, and monitor for signs and symptoms appropriately.
• Allergic reaction (onset <15 min): Mild skin itching or hives <25% body, Temp 38°C (100.4°F) or change of >1°C (>2°F) from
pre-transfusion value, chills, and hives/rash >25% body
• Febrile transfusion reaction: Temp 38°C (100.4°F) or change of >1°C (<1.8°F) from pre-transfusion value, chills, headache, facial
flushing, palpitations, cough, chest tightness, increased pulse rate and/or flank pain
• Hemolytic transfusion mentions: Immediate lysis of transfused blood can result in fever and/or tachycardia. Other symptoms
can include chills, back/flank pain, nausea/vomiting, dyspnea, flushing, bleeding, and/or hypotension. Begin aggressive NS 0.9%
treatment.
• Dilutional thrombocytopenia: This is generally not seen with infusion of 1–2 units unless patient has pre-existing thrombocytopenia
or disseminated intravascular coagulation.
• Potassium intoxication (hyperkalemia): Symptoms can include flaccidity, muscle twitching, bradycardia, EKG changes (tall peaked
T waves, prolonged P-R interval, absent P waves, prolonged QRS) and/or cardiac arrest.
• Hypoglycemia (from citrate toxicity that binds Ca): Symptoms can include arrhythmias, hypotension, muscle cramping, nausea,
vomiting, seizure activity, and/or tingling sensation in the fingers. Patient with acute or chronic hepatic insufficiency are at a
relatively higher risk of citrate toxicity. To avoid, administer PRBC at a minimum rate of >5 minute. Treatment with Calcium
Gluconate 1gm infused slowly in a different IV/IO line.
• Contact Medical Control for additional boluses as necessary.
SBP = systolic blood pressure, HR = heart rate, IV = intravenous, IO = intraosseous, pRBC = packed red blood cells, FFP = fresh frozen
plasms, U = unit
48 | JSOM Volume 23, Edition 1 / Spring 2023