
Page 72 - 2020 JSOM Winter
P. 72
/percutaneous-cricothyrotomy-quicktrach/). After equipment TABLE 1 Demographics of Participants
setup, we asked medics to verbally indicate when they were Median Age, y 32 (IQR 26–38)
ready for the time to begin. We defined an attempt as insertion Demographics Male 82% (52)
of the tube into any part of the mannequin with full removal Rank E3 6% (4)
prior to the next attempt – we did not count adjustments made
upon insertion as additional attempts. We stopped time when E4 22% (14)
the participant verbally confirmed satisfaction with place- E5 17% (11)
ment. Study team members who were either physicians board E6 41% (26)
certified in Emergency Medicine or certified registered nurse E7 13% (8)
anesthetists then confirmed correct placement via direct visu- Military experience Years since AIT 7 (IQR 3–13)
alization, insufflation, and palpation. Yes 51% (32)
Deployment experience
Months 5 (0–18)
Statistical Analysis IQR = interquartile range; AIT= advanced individual training.
We entered all data collection form data into an Excel (Micro-
soft; www.microsoft.com) database. We exported all data TABLE 2 Device Placement Data
for analysis into JMP Statistical Discovery from Statistical iGel Cricothyrotomy P Value
Analysis Software (SAS) (SAS; www.jmp.com). We compared First-pass success 68.2% (43) 69.8% (44) .847
participant characteristics based upon the technique sequence
to which they were assigned by randomization. Our primary Successful 73.0% (46) 82.5% (52) .198
cannulation
analysis was first-pass placement success between the iGel and Time to 21.8 (17.0–26.5) 63.8 (56.1–71.6) <.001
the cricothyrotomy. We also compared time to successful can- placement, s*
nulation among all participants utilizing a time-to-event anal- *Mean, 95% confidence interval.
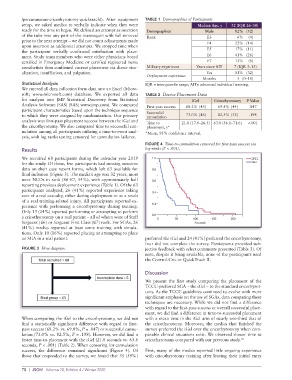
ysis, with log ranks testing censored for cannulation failures.
FIGURE 4 Time-to-cannulation censored for first-pass success via
Results log-ranks (P < .001).
We recruited 68 participants during the calendar year 2019
for the study. Of those, five participants had missing outcome
data on their case report forms, which left 63 available for
final inclusion (Figure 3). The median age was 32 years, most
were NCOs in rank (E6-E7, 54%), with approximately half
reporting previous deployment experience (Table 1). Of the 63
participants analyzed, 26 (41%) reported experience taking
care of a real casualty, either during deployment or as a result
of a real training-related injury. All participants reported ex-
perience with performing a cricothyrotomy during training.
Only 15 (24%) reported performing or attempting to perform
a cricothyrotomy on a real patient – all of whom were of Staff
Sergeant (E6) or Sergeant First Class (E7) rank. For SGAs, 26
(41%) medics reported at least some training with simula-
tions. Only 10 (16%) reported placing or attempting to place
an SGA in a real patient. preferred the iGel and 24 (41%) preferred the cricothyrotomy;
four did not complete the survey. Participants provided sub-
FIGURE 3 Flow diagram. jective feedback with select comments presented (Table 3). Of
note, despite it being available, none of the participants used
the Control-Cric or QuickTrach II.
Discussion
We present the first study comparing the placement of the
TCCC-preferred SGA – the iGel – to the standard cricothyrot-
omy. As the TCCC guidelines continued to evolve with more
significant emphasis on the use of SGAs, data comparing these
techniques are necessary. While we did not find a difference
with regard to the first-pass success or overall successful place-
ment, we did find a difference in time-to-successful placement
When comparing the iGel to the cricothyrotomy, we did not with a mean time in the iGel arm of nearly one-third that of
find a statistically significant difference with regard to first- the cricothyrotomy. Moreover, the medics that finished the
pass success (68.2% vs. 69.8%, P = .847) or successful cannu- survey preferred the iGel over the cricothyrotomy when com-
lation (73.0% vs. 82.5%, P = .198). However, we did find a parable clinical situations exist. We observed slower time to
faster time-to-placement with the iGel (21.8 seconds vs. 63.8 cricothyrotomy compared with our previous study. 10
seconds, P < .001) (Table 2). When censoring for cannulation
success, the difference remained significant (Figure 4). Of First, many of the medics reported little ongoing experience
those that responded to the survey, we found that 35 (59%) with cricothyrotomy training after leaving their initial entry
70 | JSOM Volume 20, Edition 4 / Winter 2020