
Page 94 - JSOM Spring 2020
P. 94
Methods Results
Search Strategy and Selection Criteria We examined a total of 262 studies, of which 18 were included
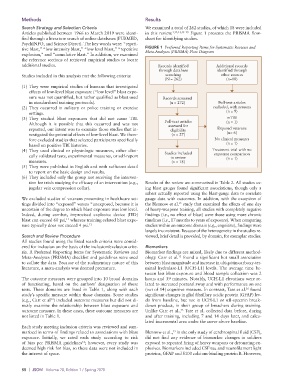
Articles published between 1966 to March 2019 were identi- in this review. 1,12,13,15–29 Figure 1 presents the PRISMA flow-
fied through a literature search of online databases (PUBMED, chart for identifying studies.
PsychINFO, and Science Direct). The key words were: “repeti-
tive blast,” “low intensity blast,” “low level blast,” “repetitive FIGURE 1 Preferred Reporting Items for Systematic Reviews and
explosion,” and “cumulative blast.” In addition, we examined Meta-Analyses (PRISMA) Flow Diagram
the reference sections of retrieved empirical studies to locate
additional studies. Records identified Additional records
through database identified through
Studies included in this analysis met the following criteria: searching other sources
(N = 262) (n=10)
(1) They were empirical studies of humans that investigated
effects of low-level blast exposure (“low level” blast expo-
sure was not quantified, but rather qualified as blast used Records screened
in standardized training protocols). (n = 272) Full-text articles
(2) They occurred in military or police training or exercise excluded, with reasons
settings. (n = 9)
(3) They studied blast exposures that did not cause TBI. mTBI
Although it is possible that this occurred and was not Full-text articles (n = 1)
assessed for
reported, our intent was to examine those studies that in- eligibility Exposed veterans
vestigated the potential effects of low-level blast. We there- (n = 27) (n= 6)
fore excluded studies that selected participants specifically No clinical measures
based on positive TBI histories. (n = 1)
(4) They used clinical or physiologic measures, either clini- Studies included Treatment trial with no
cally validated tests, experimental measures, or self-report in review exposure comparison
(n = 1)
measures. (n = 18)
(5) They were published in English and with sufficient detail
to report on the basic design and results.
(6) They included only the group not receiving the interven-
tion for trials studying the efficacy of an intervention (e.g., Results of the review are summarized in Table 2. All studies us-
jugular vein compression collar). ing blast gauges found significant associations, though only a
subset actually reported using the blast-gauge data to correlate
We excluded studies of veterans presenting in healthcare set- gauge data with outcomes. In addition, with the exception of
tings divided into “exposed” versus “unexposed, because it is the Blennow et al. study that examined the effects of one day
15
uncertain of the degree to which blast exposure was low level. of heavy-weapons training, all studies with completely negative
Indeed, during combat, improvised explosive device (IED) findings (i.e., no effect of blast) were those using more chronic
blast can exceed 60 psi, whereas training-related blast expo- timelines (i.e., 17 months to years of exposure). When comparing
11
sure typically does not exceed 4 psi. 12 studies within an outcome domain (e.g., cognitive), findings were
largely inconsistent. Because of the heterogeneity in the studies re-
Search and Review Procedure viewed, brief detail is provided, by domain, for exemplar studies.
All studies found using the listed search criteria were consid-
ered for inclusion on the basis of the inclusion/exclusion crite- Biomarkers
ria. A Preferred Reporting Items for Systematic Reviews and Biomarker findings are mixed, likely due to different method-
13
Meta-Analyses (PRISMA) checklist and guidelines were used ology. Carr et al. found a significant but small association
to collate the data. Because of the rudimentary nature of this between blast magnitude and increase in ubiquitin carboxy-ter-
literature, a meta-analysis was deemed premature. minal hydrolase-L1 (UCH-L1) levels. The average time be-
tween last blast exposure and blood sample collection was 2
The outcome measures were grouped into 10 broad domains hours and 39 minutes. Notably, UCH-L1 elevations were re-
of functioning, based on the authors’ designation of those lated to increased postural sway and with performance on one
16
tests. These domains are listed in Table 1, along with each (out of 14) cognitive measure. In contrast, Tate et al. found
study’s specific measure within those domains. Some studies significant changes in glial fibrillary acidic protein (GFAP) lev-
(e.g., Carr et al ) included outcome measures but did not di- els from baseline, but not in UCH-L1 or αII- spectrin break-
13
rectly examine the relationship between blast exposure and down product, in their group of breachers during training.
13
outcome measure. In these cases, these outcome measures are Unlike Carr et al., Tate et al. collected data before, during
not listed in Table 1. and after training, including 7 and 14 days later, and calcu-
lated incremental area under the curve above baseline.
Each study meeting inclusion criteria was reviewed and sum-
15
marized in terms of findings related to associations with blast Blennow et al., in the only study of cerebrospinal fluid (CSF),
exposure. Initially, we rated each study according to risk did not find any evidence of biomarker changes in soldiers
14
of bias per PRISMA guidelines ; however, every study was exposed to repeated firing of heavy weapons or detonating ex-
deemed high risk for bias, so these data were not included in plosives. Biomarkers included CSF tau and neurofilament light
the interest of space. proteins, GFAP and S100 calcium-binding protein B. However,
88 | JSOM Volume 20, Edition 1 / Spring 2020