
Page 42 - JSOM Spring 2020
P. 42
Spo in the mid to upper 90s on room air. Cardiovascular ex- Again, this coincided with conversion to normal sinus rhythm
2
amination revealed no murmurs/rubs/gallops, JVD, or periph- with heart rate in the 70s (Figure 2).
eral edema. His pulmonary, abdominal, skin, and neurologic
examinations were normal. Bedside electrocardiogram (ECG) The normal saline fluid bolus was completed in less than 1 hour,
showed narrow complex tachycardia with intermittent atrial and the patient stated the he felt significantly improved without
flutter (Figure 1). An 18-gauge peripheral intravenous line was any symptoms, specifically no palpitations, shortness of breath,
started in the right antecubital vein, and 1L of normal saline dizziness, or fatigue. He was advised to avoid caffeine intake, to
was initiated. Valsalva was performed by having the patient limit nicotine, and to ensure aggressive oral hydration. Repeat
attempt to exhale against closed glottis, which coincided with evaluation with ECG 14 hours later showed continued normal
conversion to normal sinus rhythm, with a heart rate in the sinus rhythm and no recurrence of symptoms (Figure 3). Daily
70s on the cardiac monitor. Upon cessation, rhythm returned follow-up over the next week was consistent with the same and
to intermittent flutter pattern similar to the initial ECG. Af- the patient noted removal of caffeine from his intake, increased
ter ensuring there was no carotid bruit, carotid massage was oral hydration, and decreased tobacco use to the previous base-
performed with similar results, and the patient stated that this line level. Due to the medical care setting with limited resources
made him feel like his heart “shifted into a smoother gear.” and no laboratory or radiology services, no further laboratory
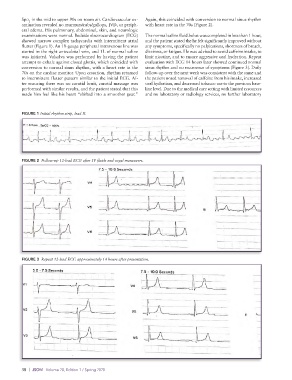
FIGURE 1 Initial rhythm strip, lead II.
FIGURE 2 Follow-up 12-lead ECG after IV fluids and vagal maneuvers.
FIGURE 3 Repeat 12-lead ECG approximately 14 hours after presentation.
38 | JSOM Volume 20, Edition 1 / Spring 2020