
Page 20 - JSOM Spring 2018
P. 20
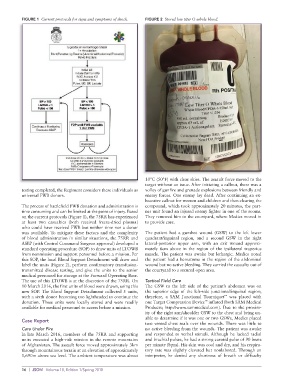
FIGURE 1 Current protocols for signs and symptoms of shock. FIGURE 2 Stored low titer O whole blood.
10°C (50°F) with clear skies. The assault force moved to the
target without an issue. After initiating a callout, there was a
testing completed, the Regiment considers these individuals as volley of gunfire and grenade explosions between friendly and
universal FWB donors. enemy forces. One enemy lay dead. After continuing an ex-
haustive callout for women and children and then clearing the
The process of battlefield FWB donation and administration is compound, which took approximately 20 minutes, the part-
time consuming and can be limited at the point of injury. Based ner unit found an injured enemy fighter in one of the rooms.
on the current protocols (Figure 1), the 75RR has experienced They removed him to the courtyard, where Medics moved in
at least two casualties (both received freeze-dried plasma) to provide care.
who could have received FWB but neither time nor a donor
was available. To mitigate these factors and the complexity The patient had a gunshot wound (GSW) to the left lower
of blood administration in similar situations, the 75RR and quadrant/inguinal region, and a second GSW in the right
ASBP (with Central Command Surgeon approval) developed a lateral-posterior upper arm, with an exit wound approxi-
standard operating procedure (SOP) to draw units of LTOWB mately 6cm above in the region of the ipsilateral trapezius
from nonmission and support personnel before a mission. Per muscle. The patient was awake but lethargic. Medics noted
this SOP, the local Blood Support Detachment will draw and the patient had a hematoma in the region of the abdominal
label the units (Figure 2), perform confirmatory transfusion- wound but no active bleeding. They carried the casualty out of
transmitted disease testing, and give the units to the senior the courtyard to a secured open area.
medical personnel for storage at the Forward Operating Base.
The use of this LTOWB is at the discretion of the 75RR. On Tactical Field Care
10 March 2016, the first units of blood were drawn, using this The GSW to the left side of the patient’s abdomen was on
new SOP. The Blood Support Detachment collected 5 units, the superior edge of the left-side junctional/inguinal region;
™
with a sixth donor becoming too lightheaded to continue the therefore, a SAM Junctional Tourniquet was placed with
™
donation. These units were locally stored and were readily one Target Compression Device inflated (both SAM Medical
available for medical personnel to access before a mission. Products; http://www.sammedical.com). Due to the proxim-
ity of the right arm/shoulder GSW to the chest and being un-
able to determine if it was one or two GSWs, Medics placed
Case Report
two vented chest seals over the wounds. There was little to
Care Under Fire no active bleeding from the wounds. The patient was awake
In late March 2016, members of the 75RR and supporting and responded to verbal stimuli. Although he lacked radial
units executed a high-risk mission in the remote mountains and brachial pulses, he had a strong carotid pulse of 90 beats
of Afghanistan. The assault force moved approximately 3km per minute (bpm). His skin was cool and dry, and his respira-
through mountainous terrain at an elevation of approximately tory rate was slightly elevated but nonlabored. Through an
1,690m above sea level. The ambient temperature was about interpreter, he denied any shortness of breath or difficulty
16 | JSOM Volume 18, Edition 1/Spring 2018