
Page 106 - Journal of Special Operations Medicine - Winter 2016
P. 106
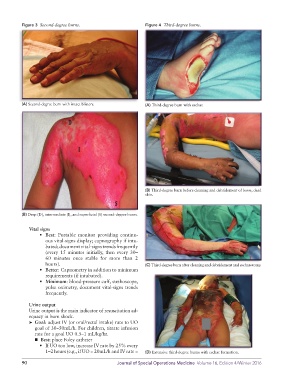
Figure 3 Second-degree burns. Figure 4 Third-degree burns.
(A) Second-degree burn with intact blisters. (A) Third-degree burn with eschar.
(B) Third-degree burn before cleaning and debridement of loose, dead
skin.
(B) Deep (D), intermediate (I), and superficial (S) second-degree burns.
Vital signs
• Best: Portable monitor providing continu-
ous vital-signs display; capnography if intu-
bated; document vital-signs trends frequently
(every 15 minutes initially, then every 30–
60 minutes once stable for more than 2
hours). (C) Third-degree burn after cleaning and debridement and escharotomy.
• Better: Capnometry in addition to minimum
requirements (if intubated).
• Minimum: blood-pressure cuff, stethoscope,
pulse oximetry, document vital-signs trends
frequently.
Urine output
Urine output is the main indicator of resuscitation ad-
equacy in burn shock.
➤ Goal: adjust IV (or oral/rectal intake) rate to UO
goal of 30–50mL/h. For children, titrate infusion
rate for a goal UO 0.5–1 mL/kg/hr.
■ Best: place Foley catheter
• If UO too low, increase IV rate by 25% every
1–2 hours (e.g., if UO = 20mL/h and IV rate = (D) Extensive third-degree burns with eschar formation.
90 Journal of Special Operations Medicine Volume 16, Edition 4/Winter 2016