
Page 21 - Journal of Special Operations Medicine - Fall 2016
P. 21
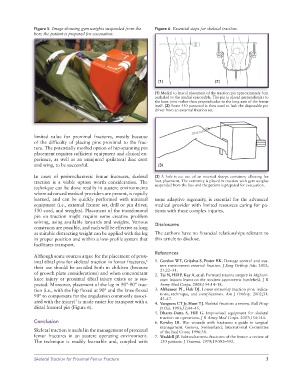
Figure 5 Image showing gym weights suspended from the Figure 6 Essential steps for skeletal traction.
box; the patient is prepared for evacuation.
(1) (2)
(1) Medial to lateral placement of the traction pin approximately 3cm
cephalad to the medial epicondyle. The pin is placed perpendicular to
the knee joint rather than perpendicular to the long axis of the femur
itself. (2) Some 550 paracord is then used to lash the disposable pin
driver from an external fixation set.
limited value for proximal fractures, mostly because
of the difficulty of placing pins proximal to the frac-
ture. The potentially morbid option of hip-spanning pin
placement requires sufficient equipment and clinical ex-
perience, as well as an uninjured ipsilateral iliac crest
and wing, to be successful. (3)
In cases of peritrochanteric femur fractures, skeletal (3) A hole is cut out of an inverted sharps container, allowing for
traction is a viable option worth consideration. The foot placement. The extremity is placed in traction with gym weights
technique can be done readily in austere environments suspended from the box and the patient is prepared for evacuation.
where advanced medical providers are present, is rapidly
learned, and can be quickly performed with minimal some adaptive ingenuity, is essential for the advanced
equipment (i.e., external fixator set, drill or pin driver, medical provider with limited resources caring for pa-
550 cord, and weights). Placement of the transfemoral tients with these complex injuries.
pin on traction might require some creative problem
solving, using available lanyards and weights. Various Disclosures
constructs are possible, and each will be effective as long
as suitable distracting weight can be applied with the leg The authors have no financial relationships relevant to
in proper position and within a low-profile system that this article to disclose.
facilitates transport.
References
Although some sources argue for the placement of prox-
imal tibial pins for skeletal traction in femur fractures, 1. Gordon WT, Grijalva S, Potter BK. Damage control and aus-
6
their use should be avoided both in children (because tere environment external fixation. J Surg Orthop Adv. 2012;
21:22–31.
of growth plate considerations) and when concomitant 2. Tai N, Hill P, Kay A, et al. Forward trauma surgery in Afghani-
knee injury or proximal tibial injury exists or is sus- stan: lessons learnt on the modern asymmetric battlefield. J R
pected. Moreover, placement of the leg in 90°-90° trac- Army Med Corps. 2008;154:14–18.
tion (i.e., with the hip flexed at 90° and the knee flexed 3. Althausen PL, Hak DJ. Lower extremity traction pins: indica-
90° to compensate for the angulation commonly associ- tions, technique, and complications. Am J Orthop. 2002;31:
43–47.
7
ated with the injury) is made easier for transport with a 4. Vangness CT Jr, Hunt TJ. Skeletal fixation: a review. Bull Hosp
distal femoral pin (Figure 6). Jt Dis. 1993;52:44–45.
5. Dharm-Datta S, Hill G. Improvised equipment for skeletal
traction on operations. J R Army Med Corps. 2007;154:144.
Conclusion 6. Rowley DI. War wounds with fractures: a guide to surgical
management. Geneva, Switzerland; International Committee
Skeletal traction is useful in the management of proximal of the Red Cross; 1996:38.
femur fractures in an austere operating environment. 7. Waddell JP. Subtrochanteric fractures of the femur: a review of
The technique is readily learnable and, coupled with 130 patients. J Trauma. 1979;19:582–592.
Skeletal Traction for Proximal Femur Fracture 3