
Page 120 - Journal of Special Operations Medicine - Summer 2016
P. 120
working to move this from a pilot project to an endur- and critical casualties in austere environments. Go to
ing program. the website, PFCare.org, and the SOMA website, www
.specialoperationsmedicine.org to read, learn, and com-
Other newly formed Sub-Working Groups include In- ment. Ultimately, we hope to improve your knowledge
formation Management (SFC Paul Loos, 18D, the Man base, and maximize medical care to our patients in dif-
behind PFCare.org); Research (MAJ Doug Powell, MD); ficult operational situations.
Training (CPT Andrew Schaffrinna, MD); Strategic Mes-
saging (LTC Jamie Riesberg, MD); and Education (Maj COL Keenan is a board-certified emergency medicine physi-
Jo Schmid, RN; CANSOF). Each of these coordinators cian, and is currently serving as Command Surgeon, Special
will tackle projects with the help of multiple SMEs who Operations Command, Europe. He has previously served as
have regularly contributed to the successes of the WG Battalion Surgeon in both 1st and 3rd SFG(A), and as Group
Surgeon, 10th SFG(A). He is the coordinator for the SOCOM
over the past 2.5 years.
Prolonged Field Care Working Group.
E-mail: sean.keenan1.mil@mail.mil.
We’re excited to move forward to identify and address
knowledge and training gaps in the SOF medical com-
munity, specifically with the provision of care to serious
William H. Poston; 18D, Katarzyna (Kasia) Hampton, MD
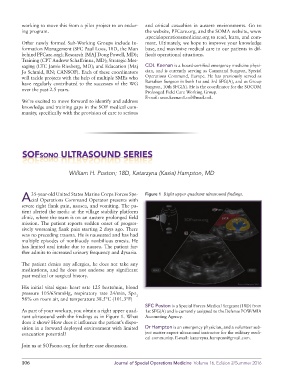
35-year-old United States Marine Corps Forces Spe- Figure 1 Right upper quadrant ultrasound findings.
A cial Operations Command Operator presents with
severe right flank pain, nausea, and vomiting. The pa-
tient alerted the medic at the village stability platform
clinic, where the team is on an austere prolonged field
mission. The patient reports sudden onset of progres-
sively worsening flank pain starting 2 days ago. There
was no preceding trauma. He is nauseated and has had
multiple episodes of nonbloody nonbilious emesis. He
has limited oral intake due to nausea. The patient fur-
ther admits to increased urinary frequency and dysuria.
The patient denies any allergies, he does not take any
medications, and he does not endorse any significant
past medical or surgical history.
His initial vital signs: heart rate 125 beats/min, blood
pressure 105/65mmHg, respiratory rate 24/min, Spo
2
98% on room air, and temperature 38.5°C (101.3°F)
SFC Poston is a Special Forces Medical Sergeant (18D) from
As part of your workup, you obtain a right upper quad- 1st SFG(A) and is currently assigned to the Defense POW/MIA
rant ultrasound with the findings as in Figure 1. What Accounting Agency.
does it show? How does it influence the patient’s dispo-
sition in a forward deployed environment with limited Dr Hampton is an emergency physician, and a volunteer sub-
evacuation potential? ject matter expert ultrasound instructor for the military medi-
cal community. E-mail: katarzyna.hampton@gmail.com.
Join us at SOFsono.org for further case discussion.
106 Journal of Special Operations Medicine Volume 16, Edition 2/Summer 2016