
Page 18 - Journal of Special Operations Medicine - Fall 2015
P. 18
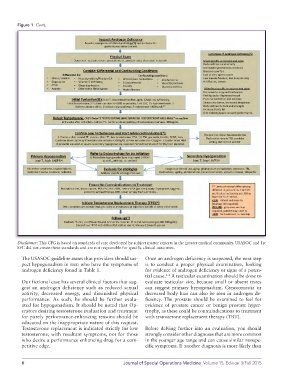
Figure 1 Cont.
Disclaimer: This CPG is based on standards of care developed by subject matter experts in the greater medical community. USASOC and 1st
SFC did not create these standards and are not responsible for specific clinical outcomes.
The USASOC guideline states that providers should sus- Once an androgen deficiency is suspected, the next step
pect hypogonadism in men who have the symptoms of is to conduct a proper physical examination, looking
androgen deficiency found in Table 1. for evidence of androgen deficiency or signs of a poten-
tial cause. A testicular examination should be done to
1-4
Our fictional case has several clinical factors that sug- evaluate testicular size, because small or absent testes
gest an androgen deficiency such as reduced sexual can suggest primary hypogonadism. Gynecomastia or
activity, decreased energy, and diminished physical decreased body hair can also be seen in androgen de-
performance. As such, he should be further evalu- ficiency. The prostate should be examined to feel for
ated for hypogonadism. It should be noted that Op- evidence of prostate cancer or benign prostate hyper-
erators desiring testosterone evaluation and treatment trophy, as these could be contraindications to treatment
for purely performance-enhancing reasons should be with testosterone replacement therapy (TRT).
educated on the inappropriate nature of this request.
Testosterone replacement is indicated strictly for low Before delving further into an evaluation, you should
testosterone, with resultant symptoms, not for those strongly consider other diagnoses that are more common
who desire a performance enhancing drug for a com- in the younger age range and can cause similar nonspe-
petitive edge. cific symptoms. If another diagnosis is more likely than
6 Journal of Special Operations Medicine Volume 15, Edition 3/Fall 2015