
Page 17 - Journal of Special Operations Medicine - Fall 2015
P. 17
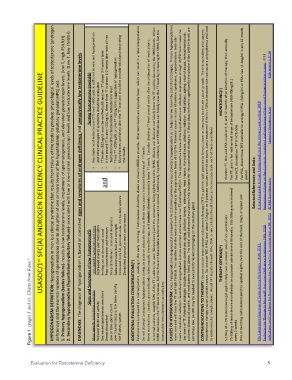
HYPOGONADISM DEFINITION: Hypogonadism in men is a clinical syndrome that results from failure of the tes6s to produce physiological levels of testosterone (androgen
2. Secondary hypogonadism (hypothalamic-‐pituitary failure)-‐ associated with low or low-‐normal gonadotropin levels and low testosterone levels. (Low T, low FSH/LH)
1. Primary hypogonadism (testes failure)-‐ results in low testosterone levels, impairment of spermatogenesis, and elevated gonadotropin levels. (low T, high FSH/LH)
DIAGNOSIS: The diagnosis of hypogonadism is based on consistent signs and symptoms of androgen deficiency and unequivocally low testosterone levels.
FDA warning 2014
USASOC/1 st SFC(A) ANDROGEN DEFICIENCY CLINICAL PRACTICE GUIDELINE
TesXng Testosterone Levels(&) Any single total testosterone (TT) level >300ng/dL is sufficient to rule out hypogonadism and other e6ologies of symptoms should be evaluated TT levels <300ng/dL must be verified with another TT drawn 2-‐4 weeks later If the second TT is also <300ng/dL, then a third TT is drawn 1-‐2 weeks later with a Free Testosterone (FT) or bioavailable test
deficiency) and the normal number of spermatozoa due to disrup6on of one or more levels of the hypothalamic-‐pituitary-‐gonadal (HPG) axis.
• • • • • the results. For HCT, discon6nue TRT if HCT>50% period A prac6cal guide to male hypogonadism in the primary care sefng. 2010
and Testosterone is released in a diurnal paPern, peaking in the early morning. Testosterone should be drawn as close to 0800 as possible. ATernoon levels are typically lower which can result in a false interpreta6on Some medica6ons ; opiates, glucocor6coids, ketoconazole, chemotherapy, and anabolic steroids transiently lower TT levels. Consider checking TT level
Signs and Symptoms of Low Testosterone($) Less specific symptoms and signs Decreased energy and mo6va6on Feeling sad or depressed mood Poor concentra6on and memory Sleep disturbance, increased sleepiness Reduced muscle bulk and strength Increased body fat, gynecomas6a, dec tes6cle volume Diminished physical or work performance Do not aPempt to diagnosis hypogonadism during an
Figure 1 (pages 5 and 6). Charts from Kane. 1
More specific symptoms and signs Reduced libido and ac6vity Decreased spontaneous erec6ons Breast discomfort Low or zero sperm count Low trauma fracture, low bone density Hot flushes, sweats ADDITIONAL EVALUATION CONSIDERATIONS(*) bioavailable testosterone is actually low. every 2 weeks The Laboratory Diagnosis of Testosterone Deficiency -‐ AUA. 2013.
Evaluation for Testosterone Deficiency 5