
Page 62 - Journal of Special Operations Medicine - Spring 2015
P. 62
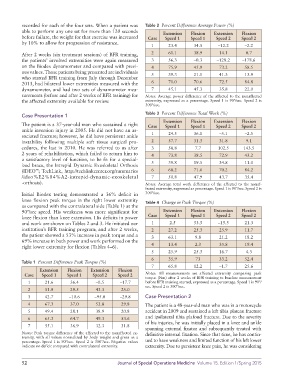
recorded for each of the four sets. When a patient was Table 2 Percent Difference Average Power (%)
able to perform any one set for more than 120 seconds Extension Flexion Extension Flexion
before failure, the weight for that exercise was increased Case Speed 1 Speed 1 Speed 2 Speed 2
by 10% to allow for progression of resistance.
1 23.4 34.5 –12.2 –2.2
After 2 weeks (six treatment sessions) of BFR training, 2 61.1 38.9 14.1 0.7
the patients’ involved extremities were again measured 3 56.3 –0.3 –128.2 –178.6
on the Biodex dynamometer and compared with previ 4 75.9 45.9 73.2 58.5
ous values. Those patients being presented are individuals 5 39.3 21.1 41.3 13.9
who started BFR training from July through December
2013, had bilateral lower extremities measured with the 6 71.0 70.6 72.5 84.8
dynamometer, and had two sets of dynamometer mea 7 45.1 45.3 35.8 22.0
surements (before and after 2 weeks of BFR training) for Notes: Average power difference of the affected to the nonaffected
the affected extremity available for review. extremity, expressed as a percentage. Speed 1 is 90º/sec. Speed 2 is
300º/sec.
Case Presentation 1 Table 3 Percent Difference Total Work (%)
Extension Flexion Extension Flexion
The patient is a 37yearold man who sustained a right Case Speed 1 Speed 1 Speed 2 Speed 2
ankle inversion injury in 2005. He did not have an as
sociated fracture; however, he did have persistent ankle 1 24.5 36.1 –5.1 –2.5
instability following multiple soft tissue surgical pro 2 57.7 31.3 31.8 9.1
cedures, the last in 2010. He was referred to us after 3 58.8 7.7 102.5 143.5
2 years of rehabilitation, which failed to return him to 4 73.8 38.5 72.9 43.2
a satisfactory level of function, to be fit for a special 5 39.8 19.5 34.8 11.0
ized brace, the Intrepid Dynamic Exoskeletal Orthosis
(IDEO ; TechLink, http://techlinkcenter.org/summaries 6 68.2 71.6 70.2 84.2
™
/ideo%E2%84%A2intrepiddynamicexoskeletal 7 50.8 47.9 43.7 35.4
orthosis). Notes: Average total work difference of the affected to the nonaf
fected extremity, expressed as percentage. Speed 1 is 90º/sec. Speed 2 is
Initial Biodex testing demonstrated a 36% deficit in 300º/sec.
knee flexion peak torque in the right lower extremity Table 4 Change in Peak Torque (%)
as compared with the contralateral side (Table 1) at the
90º/sec speed. His weakness was more significant for Extension Flexion Extension Flexion
knee flexion than knee extension. His deficits in power Case Speed 1 Speed 1 Speed 2 Speed 2
and work are shown on Tables 2 and 3. He initiated our 1 2.5 53.5 –15.3 21.3
institution’s BFR training program; and after 2 weeks, 2 27.2 25.3 25.9 11.7
the patient showed a 53% increase in peak torque and a 3 63.1 9.8 21.2 18.2
69% increase in both power and work performed on the
right lower extremity for flexion (Tables 4–6). 4 13.4 2.3 35.8 19.4
5 25.9 25.3 16.7 4.3
6 35.9 73 33.2 52.4
Table 1 Percent Difference Peak Torque (%)
7 65.8 12.2 –1.7 25.6
Extension Flexion Extension Flexion
Case Speed 1 Speed 1 Speed 2 Speed 2 Notes: All measurements are affected extremity comparing peak
torque (Nm) after 2 weeks of BFR training to baseline measurement
1 21.6 36.4 –0.5 –17.7 before BFR training started, expressed as a percentage. Speed 1 is 90º/
sec. Speed 2 is 300º/sec.
2 51.9 29.5 43.3 25.0
3 42.7 –10.6 –95.0 –29.8 Case Presentation 2
4 67.3 37.0 53.8 29.8 The patient is a 48yearold man who was in a motorcycle
5 49.4 28.1 38.9 20.8 accident in 2009 and sustained a left tibia plateau fracture
6 65.3 64.7 49.3 53.6 and ipsilateral tibia plafond fracture. Due to the severity
of his injuries, he was initially placed in a knee and ankle
7 55.1 36.9 32.3 31.8
spanning external fixator and subsequently treated with
Notes: Peak torque difference of the affected to the nonaffected ex definitive internal fixation. Since that time, he has contin
tremity, with all values normalized by body weight and given as a
percentage. Speed 1 is 90º/sec. Speed 2 is 300º/sec. Negative values ued to have weakness and limited function of his left lower
indicate no deficit compared with contralateral extremity. extremity. Due to persistent knee pain, he was considering
52 Journal of Special Operations Medicine Volume 15, Edition 1/Spring 2015