
Page 36 - Journal of Special Operations Medicine - Spring 2015
P. 36
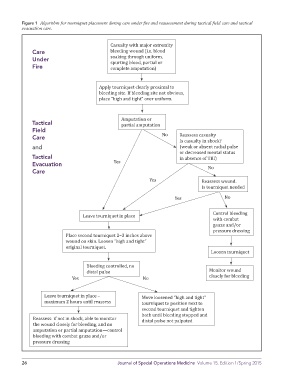
Figure 1 Algorithm for tourniquet placement during care under fire and reassessment during tactical field care and tactical
evacuation care.
Casualty with major extremity
Care bleeding wound (i.e. blood
Under soaking through uniform,
Fire spurting blood, partial or
complete amputation)
Apply tourniquet clearly proximal to
bleeding site. If bleeding site not obvious,
place “high and tight” over uniform.
Tactical Amputation or
partial amputation
Field
Care No Reassess casualty
Is casualty in shock?
and (weak or absent radial pulse
or decreased mental status
Tactical in absence of TBI)
Evacuation Yes
No
Care
Yes Reassess wound.
Is tourniquet needed
Yes No
Control bleeding
Leave tourniquet in place
with combat
gauze and/or
pressure dressing
Place second tourniquet 2–3 inches above
wound on skin. Loosen “high and tight”
original tourniquet.
Loosen tourniquet
Bleeding controlled, no
Monitor wound
distal pulse
closely for bleeding
Yes No
Leave tourniquet in place – Move loosened “high and tight”
maximum 2 hours until reassess tourniquet to position next to
second tourniquet and tighten
both until bleeding stopped and
Reassess: if not in shock, able to monitor
distal pulse not palpated
the wound closely for bleeding, and no
amputation or partial amputation—control
bleeding with combat gauze and/or
pressure dressing
26 Journal of Special Operations Medicine Volume 15, Edition 1/Spring 2015