
Page 10 - Journal of Special Operations Medicine - Fall 2014
P. 10
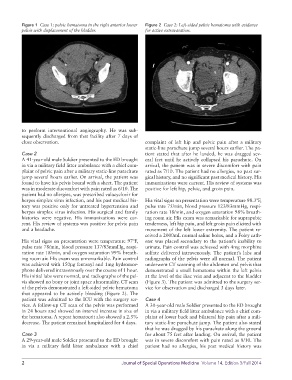
Figure 1 Case 1: pelvic hematoma in the right anterior lower Figure 2 Case 2: Left-sided pelvic hematoma with evidence
pelvis with displacement of the bladder. for active extravasation.
to perform interventional angiography. He was sub-
sequently discharged from that facility after 7 days of
close observation. complaint of left hip and pelvic pain after a military
static-line parachute jump several hours earlier. The pa-
Case 2 tient stated that after he landed, he was dragged sev-
A 41-year-old male Soldier presented to the ED brought eral feet until he actively collapsed his parachute. On
in via a military field litter ambulance with a chief com- arrival, the patient was in severe discomfort with pain
plaint of pelvic pain after a military static-line parachute rated as 7/10. The patient had no allergies, no past sur-
jump several hours earlier. On arrival, the patient was gical history, and no significant past medical history. His
found to have his pelvis bound with a sheet. The patient immunizations were current. His review of systems was
was in moderate discomfort with pain rated as 6/10. The positive for left hip, pelvic, and groin pain.
patient had no allergies, was prescribed valacyclovir for
herpes simplex virus infection, and his past medical his- His vital signs on presentation were temperature 98.3ºF,
tory was positive only for untreated hypertension and pulse rate 75/min, blood pressure 123/83mmHg, respi-
herpes simplex virus infection. His surgical and family ration rate 18/min, and oxygen saturation 98% breath-
histories were negative. His immunizations were cur- ing room air. His exam was remarkable for suprapubic
rent. His review of systems was positive for pelvic pain tenderness, left hip pain, and left groin pain elicited with
and a headache. movement of the left lower extremity. The patient re-
ceived a 2000mL normal saline bolus, and a Foley cath-
His vital signs on presentation were temperature 97ºF, eter was placed secondary to the patient’s inability to
pulse rate 78/min, blood pressure 137/83mmHg, respi- urinate. Pain control was achieved with 4mg morphine
ration rate 18/min, and oxygen saturation 99% breath- sulfate delivered intravenously. The patient’s labs and
ing room air. His exam was unremarkable. Pain control radiographs of the pelvis were all normal. The patient
was achieved with 150μg fentanyl and 1mg hydromor- underwent CT scanning of the abdomen and pelvis that
phone delivered intravenously over the course of 1 hour. demonstrated a small hematoma within the left pelvis
His initial labs were normal, and radiographs of the pel- at the level of the iliac vein and adjacent to the bladder
vis showed no bony or joint space abnormality. CT scan (Figure 3). The patient was admitted to the surgery ser-
of the pelvis demonstrated a left-sided pelvic hematoma vice for observation and discharged 3 days later.
that appeared to be actively bleeding (Figure 2). The
patient was admitted to the ICU with the surgery ser- Case 4
vice. A follow-up CT scan of the pelvis was performed A 30-year-old male Soldier presented to the ED brought
in 24 hours and showed an interval increase in size of in via a military field litter ambulance with a chief com-
the hematoma. A repeat hematocrit also showed a 2.5% plaint of lower back and bilateral hip pain after a mili-
decrease. The patient remained hospitalized for 4 days. tary static-line parachute jump. The patient also stated
that he was dragged by his parachute along the ground
Case 3 for about 75 feet after landing. On arrival, the patient
A 29-year-old male Soldier presented to the ED brought was in severe discomfort with pain rated as 8/10. The
in via a military field litter ambulance with a chief patient had no allergies, his past medical history was
2 Journal of Special Operations Medicine Volume 14, Edition 3/Fall 2014