
Page 45 - ATP-P 11th Ed
P. 45
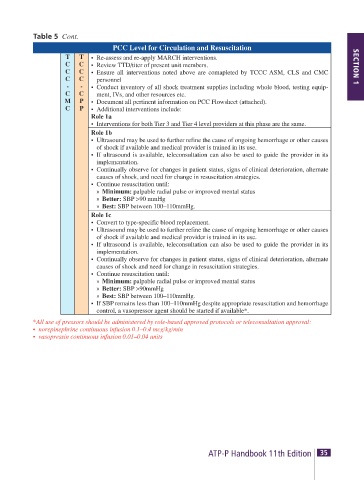
Table 5 Cont.
PCC Level for Circulation and Resuscitation
T T • Re-assess and re-apply MARCH interventions.
C C • Review TTD/titer of present unit members. SECTION 1
C C • Ensure all interventions noted above are comapleted by TCCC ASM, CLS and CMC
C C personnel
- - • Conduct inventory of all shock treatment supplies including whole blood, testing equip-
C C ment, IVs, and other resources etc.
M P • Document all pertinent information on PCC Flowsheet (attached).
C P • Additional interventions include:
Role 1a
• Interventions for both Tier 3 and Tier 4 level providers at this phase are the same.
Role 1b
• Ultrasound may be used to further refine the cause of ongoing hemorrhage or other causes
of shock if available and medical provider is trained in its use.
• If ultrasound is available, teleconsultation can also be used to guide the provider in its
implementation.
• Continually observe for changes in patient status, signs of clinical deterioration, alternate
causes of shock, and need for change in resuscitation strategies.
• Continue resuscitation until:
» Minimum: palpable radial pulse or improved mental status
» Better: SBP >90 mmHg
» Best: SBP between 100–110mmHg.
Role 1c
• Convert to type-specific blood replacement.
• Ultrasound may be used to further refine the cause of ongoing hemorrhage or other causes
of shock if available and medical provider is trained in its use.
• If ultrasound is available, teleconsultation can also be used to guide the provider in its
implementation.
• Continually observe for changes in patient status, signs of clinical deterioration, alternate
causes of shock and need for change in resuscitation strategies.
• Continue resuscitation until:
» Minimum: palpable radial pulse or improved mental status
» Better: SBP >90mmHg
» Best: SBP between 100–110mmHg.
• If SBP remains less than 100–110mmHg despite appropriate resuscitation and hemorrhage
control, a vasopressor agent should be started if available*.
*All use of pressors should be administered by role-based approved protocols or teleconsultation approval:
• norepinephrine continuous infusion 0.1–0.4 mcg/kg/min
• vasopressin continuous infusion 0.01–0.04 units
34 SECTION 1 TACTICAL TRAUMA PROTOCOLS (TTPs) ATP-P Handbook 11th Edition 35