
Page 229 - 2025 Ranger Medic Handbook
P. 229
Pediatric Tactical Combat Casualty Care Guidelines
Patient assessment and TCCC application largely remain unchanged for pediatric prehospital trauma patients, as com-
pared to adults, except for the following considerations:
Massive hemorrhage: Owing to much smaller blood volumes in children than in adults, immediate control of massive
hemorrhage is necessary to prevent hemorrhagic shock, and blood-based resuscitation must begin rapidly with any
significant loss of blood. Use tourniquets high and tight. U.S. military-approved tourniquets are effective in children with
limb circumferences ≥13cm (around 5 inches), generally children aged 2 years and over. Use of commercial windlass
tourniquets will likely require more wraps around the limb and more turns of the windlass to achieve hemostasis as
compared to adults. If the tourniquet is ineffective, use direct pressure, hemostatic gauze, and/or pressure dressings to
stop life-threatening extremity hemorrhage. If the casualty is younger than 2 years of age or has a limb circumference
< 13cm, use an improvised windlass tourniquet or elastic (ACE) bandage wrapped tightly. Circumferential and direct
manual pressure is highly recommended at arterial pressure points.
Airway: A crying pediatric casualty’s airway is intact. If the child is semiconscious or unconscious, their tongue is the
most common source of airway obstruction. The younger the child, the larger the occiput compared to the rest of the
body and the greater the importance of ensuring full head extension (by using a shoulder roll). Inadequate head exten-
sion results in airway occlusion. Although TCCC should always consider cervical spine injury in trauma, survivable
pediatric cervical spine fractures are extremely rare and should not take precedence over establishing a patent airway.
Airway adjuncts (oropharyngeal/nasopharyngeal airways) can be used to maintain a patent airway. An adult bag valve
mask (BVM) can be used for pediatric ventilatory support, but only use enough pressure to generate adequate chest
rise, which is much less than required for an adult (avoid hyper- or overinflation). In extreme circumstances, surgical
cricothyroidotomy can be performed on casualties younger than 8 years old, but caution must be taken in younger chil-
dren because of immature thyroid cartilage and the small size or limited space of the cricothyroid membrane. Standard
adult cricothyroid tubes are too large to fit a pediatric trachea, but pediatric endotracheal tubes can be modified to fit
the cricothyroid membrane.
Resuscitation: Unlike in adult shock, hypotension is a late finding in the pediatric population. Children should be resus-
citated early, before the onset of hypotension. Early signs of shock (before hypotension) include tachycardia and capillary
refill ≥ 3 seconds. Signs of uncompensated shock include altered mental status, weak distal pulses, and hypotension.
Permissive hypotension after hemorrhage is NOT RECOMMENDED in children. Adequate blood-based resuscitation
should improve heart rate, respiratory rate, capillary refill, mental status, hypotension, and urine output (goal = 1mL/kg/hr).
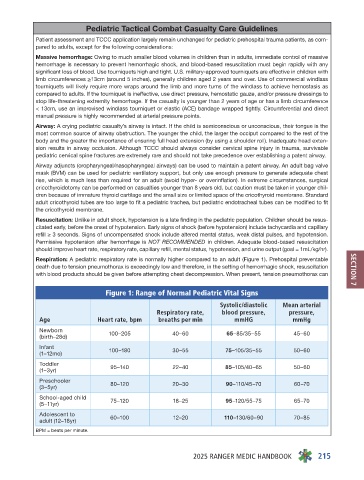
Respiration: A pediatric respiratory rate is normally higher compared to an adult (Figure 1). Prehospital preventable
death due to tension pneumothorax is exceedingly low and therefore, in the setting of hemorrhagic shock, resuscitation SECTION 7
with blood products should be given before attempting chest decompression. When present, tension pneumothorax can
Figure 1: Range of Normal Pediatric Vital Signs
Systolic/diastolic Mean arterial
Respiratory rate, blood pressure, pressure,
Age Heart rate, bpm breaths per min mmHG mmHg
Newborn
(birth–28d) 100–205 40–60 65–85/35–55 45–60
Infant 100–180 30–55 75–105/35–55 50–60
(1–12mo)
Toddler 95–140 22–40 85–105/40–65 50–60
(1–3yr)
Preschooler
(3–5yr) 80–120 20–30 90–110/45–70 60–70
School-aged child
(5–11yr) 75–120 18–25 95–120/55–75 65–70
Adolescent to 60–100 12–20 110–130/60–90 70–85
adult (12–18yr)
BPM = beats per minute.
2025 RANGER MEDIC HANDBOOK 215