
Page 48 - JSOM Spring 2026
P. 48
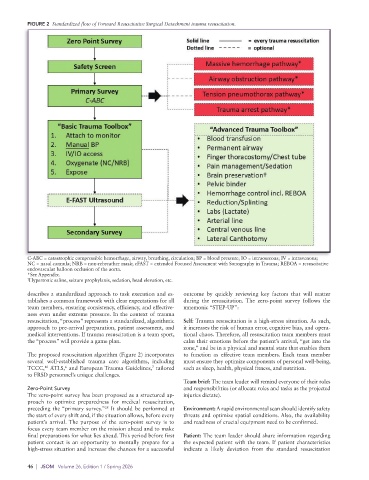
FIGURE 2 Standardized flow of Forward Resuscitative Surgical Detachment trauma resuscitation.
C-ABC = catastrophic compressible hemorrhage, airway, breathing, circulation; BP = blood pressure; IO = intraosseous; IV = intravenous;
NC = nasal cannula; NRB = non-rebreather mask; eFAST = extended Focused Assessment with Sonography in Trauma; REBOA = resuscitative
endovascular balloon occlusion of the aorta.
*See Appendix.
† Hypertonic saline, seizure prophylaxis, sedation, head elevation, etc.
describes a standardized approach to task execution and es- outcome by quickly reviewing key factors that will matter
tablishes a common framework with clear expectations for all during the resuscitation. The zero-point survey follows the
team members, ensuring consistency, efficiency, and effective- mnemonic “STEP-UP”:
ness even under extreme pressure. In the context of trauma
resuscitation, “process” represents a standardized, algorithmic Self: Trauma resuscitation is a high-stress situation. As such,
approach to pre-arrival preparation, patient assessment, and it increases the risk of human error, cognitive bias, and opera-
medical interventions. If trauma resuscitation is a team sport, tional chaos. Therefore, all resuscitation team members must
the “process” will provide a game plan. calm their emotions before the patient’s arrival, “get into the
zone,” and be in a physical and mental state that enables them
The proposed resuscitation algorithm (Figure 2) incorporates to function as effective team members. Each team member
several well-established trauma care algorithms, including must ensure they optimize components of personal well-being,
6
16
TCCC, ATLS, and European Trauma Guidelines, tailored such as sleep, health, physical fitness, and nutrition.
7
to FRSD personnel’s unique challenges.
Team brief: The team leader will remind everyone of their roles
Zero-Point Survey and responsibilities (or allocate roles and tasks as the projected
The zero-point survey has been proposed as a structured ap- injuries dictate).
proach to optimize preparedness for medical resuscitation,
preceding the “primary survey.” It should be performed at Environment: A rapid environmental scan should identify safety
28
the start of every shift and, if the situation allows, before every threats and optimize spatial conditions. Also, the availability
patient’s arrival. The purpose of the zero-point survey is to and readiness of crucial equipment need to be confirmed.
focus every team member on the mission ahead and to make
final preparations for what lies ahead. This period before first Patient: The team leader should share information regarding
patient contact is an opportunity to mentally prepare for a the expected patient with the team. If patient characteristics
high-stress situation and increase the chances for a successful indicate a likely deviation from the standard resuscitation
46 | JSOM Volume 26, Edition 1 / Spring 2026