
Page 91 - 2023 SMOG Digital
P. 91
SPECIAL POPULATIONS
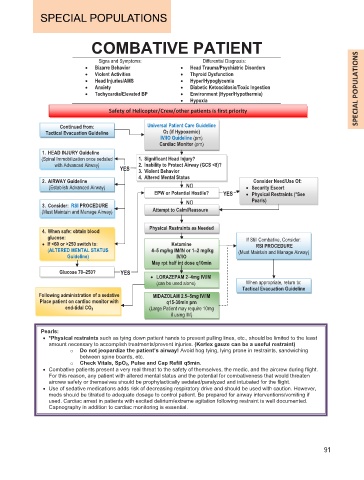
COMBATIVE PATIENT
Signs and Symptoms: Differential Diagnosis:
• Bizarre Behavior • Head Trauma/Psychiatric Disorders
• Violent Activities • Thyroid Dysfunction
• Head Injuries/AMS • Hyper/Hypoglycemia
• Anxiety • Diabetic Ketoacidosis/Toxic Ingestion
• Tachycardia/Elevated BP • Environment (Hyper/Hypothermia)
• Hypoxia
Safety of Helicopter/Crew/other patients is first priority
Continued from: Universal Patient Care Guideline
Tactical Evacuation Guideline O2 (if Hypoxemic)
IV/IO Guideline (prn)
Cardiac Monitor (prn)
1. HEAD INJURY Guideline
(Spinal Immobilization once sedated 1. Significant Head Injury?
with Advanced Airway) 2. Inability to Protect Airway (GCS <8)?
YES 3. Violent Behavior
4. Altered Mental Status
2. AIRWAY Guideline Consider Need/Use Of:
(Establish Advanced Airway) NO • Security Escort
EPW or Potential Hostile? YES • Physical Restraints (*See
3. Consider: RSI PROCEDURE NO Pearls)
(Must Maintain and Manage Airway) Attempt to Calm/Reassure
Physical Restraints as Needed
4. When safe: obtain blood
glucose: If Still Combative, Consider:
• If <6 60 or >250 switch to: Ketamine RSI PROCEDURE
(ALTERED MENTAL STATUS 4–5 mg/kg IM/IN or 1––2 mg/kg (Must Maintain and Manage Airway)
–
Guideline) IV/IO
May rpt half int dose q10min
Glucose 70––250? YES
• LORAZEPAM 2–4mg IV/IM
–
(can be used alone) When appropriate, return to:
Tactical Evacuation Guideline
Following administration of a sedative MIDAZOLAM 2.5––5mg IV/IM
Place patient on cardiac monitor with q15-30min prn
end-tidal CO 2 (Large Patient may require 10mg
if using IM)
Pearls:
• *Physical restraints such as tying down patient hands to prevent pulling lines, etc., should be limited to the least
amount necessary to accomplish treatments/prevent injuries. (Kerlex gauze can be a useful restraint)
o Do not jeopardize the patient’s airway! Avoid hog tying, lying prone in restraints, sandwiching
between spine boards, etc.
o Check Vitals, SpO2, Pulse and Cap Refill q5min.
• Combative patients present a very real threat to the safety of themselves, the medic, and the aircrew during flight.
For this reason, any patient with altered mental status and the potential for combativeness that would threaten
aircrew safety or themselves should be prophylactically sedated/paralyzed and intubated for the flight.
• Use of sedative medications adds risk of decreasing respiratory drive and should be used with caution. However,
meds should be titrated to adequate dosage to control patient. Be prepared for airway interventions/vomiting if
used. Cardiac arrest in patients with excited delirium/extreme agitation following restraint is well documented.
Capnography in addition to cardiac monitoring is essential.
91