
Page 236 - 2023 SMOG Digital
P. 236
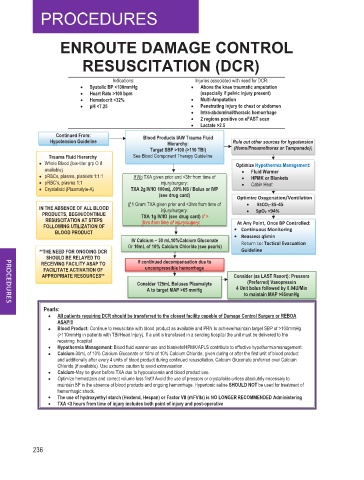
ENROUTE DAMAGE CONTROL
RESUSCITATION (DCR)
Indications: Injuries associated with need for DCR:
• Systolic BP <100mmHg • Above the knee traumatic amputation
• Heart Rate >100 bpm (especially if pelvic injury present)
• Hematocrit <32% • Multi-Amputation
• pH <7.25 • Penetrating injury to chest or abdomen
• Intra-abdominal/thoracic hemorrhage
• 2 regions positive on eFAST scan
• Lactate >2.5
Continued From: Blood Products IAW Trauma Fluid
Hypotension Guideline Hierarchy: Rule out other sources for hypotension
Target SBP >100 (>110 TBI) (Hemo/Pneumothorax or Tamponade))
Trauma Fluid Hierarchy See Blood Component Therapy Guideline
Whole Blood (low-titer grp O if Optimize Hypothermia Management:
available) • Fluid Warmer
pRBCs, plasma, platelets 1:1:1 If No TXA given prior and <3hr from time of • HPMK or Blankets
pRBC’s, plasma 1:1 injury/surgery: • Cabin Heat
g
Crystalloid (Plasmalyte-A) TXA 2g IV/IO 100mL .09% NS / Bolus or IVP
L
(see drug card) Optimize Oxygenation/Ventilation
If 1 Gram TXA given prior and <3hrs from time of • EtCO2-35-45
IN THE ABSENCE OF ALL BLOOD injury/surgery: • SpO2 >94%
PRODUCTS, BEGIN/CONTINUE TXA 1g IV/IO (see drug card) If >
g
RESUSCITATION AT STEPS 3hrs from time of injury/surgery: At Any Point, Once BP Controlled:
FOLLOWING UTILIZATION OF • Continuous Monitoring
BLOOD PRODUCT • Reassess q5min
IV Calcium – 30 mL10%Calcium Gluconate Return to: Tactical Evacuation
Or 10mL of 10% Calcium Chloride (see pearls)
**THE NEED FOR ONGOING DCR Guideline
SHOULD BE RELAYED TO
RECEIVING FACILITY ASAP TO If continued decompensation due to
FACILITATE ACTIVATION OF uncompressible hemorrhage
APPROPRIATE RESOURCES** Consider (as LAST Resort): Pressors
L
Consider 125mL Boluses Plasmalyte (Preferred) Vasopressin
A to target MAP >65 mmHg 4 Unit bolus followed by 0.04U/Min
to maintain MAP >65mmHg
Pearls:
All patients requiring DCR should be transferred to the closest facility capable of Damage Control Surgery or REBOA
ASAP!!!
Blood Product: Continue to resuscitate with blood product as available and PRN to achieve/maintain target SBP of >100mmHg
(>110mmHg in patients with TBI/Head Injury). If a unit is transfused in a sending hospital the unit must be delivered to the
receiving hospital
Hypothermia Management: Blood fluid warmer use and blankets/HPMK/APLS contribute to effective hypothermia management.
Calcium-30mL of 10% Calcium Gluconate or 10ml of 10% Calcium Chloride, given during or after the first unit of blood product
and additionally after every 4 units of blood product during continued resuscitation. Calcium Gluconate preferred over Calcium
Chloride (if available). Use extreme caution to avoid extravasation.
Calcium-May be given before TXA due to hypocalcemia and blood product use.
Optimize hemostasis and correct volume loss first!! Avoid the use of pressors or crystalloids unless absolutely necessary to
maintain BP in the absence of blood products and ongoing hemorrhage. Hypertonic saline SHOULD NOT be used for treatment of
hemorrhagic shock.
The use of hydroxyethyl starch (Hextend, Hespan) or Factor VII (rhFVIIa) is NO LONGER RECOMMENDED Administering
3
TXA <3 hours from time of injury includes both point of injury and post-operative
236