
Page 66 - PJ MED OPS Handbook 8th Ed
P. 66
Lateral Canthotomy
WARNING Do not attempt these procedures if not trained or qualified. NOT ALL PJs are taught,
or qualified, to perform this procedure. Pararescue Medical Directors will authorize prop-
erly trained Pararescuemen to perform this procedure.
Lateral canthotomy is indicated for casualties presenting with: Retrobulbar Hemorrhage (RBH)
bleeding into the orbital space which is behind the eyeball, is a vision-threatening condition causing
increased pressure behind the eye on the optic nerve leading to irreversible vision loss. It is also
known as orbital compartment syndrome. As with other compartment syndromes, the goal is to
lower the pressure as soon as possible to prevent tissue damage. Vision loss typically will occur after
approximately 90 minutes of increased pressure.
1. The first step is prompt recognition of eye injury and need for intervention
a. Severe eye pain
b. Proptosis: bulging of the affected eye compared to other eye
c. Increased intraocular pressure (IOP) by palpation (increased firmness compared to oppo-
site eye)
d. Decrease in or loss of visual acuity
2. Prevent further injury
a. Apply ice pack around the eye while avoiding direct compression of the eye
b. Activate evacuation (PRIORITY)
c. Initiate teleconsult with photos
d. Maintain patient in position with head elevated
3. If no improvement, perform lateral canthotomy as indicated as soon as possible, preferably
within 90 minutes of injury.
4. The indication for lateral canthotomy is orbital compartment syndrome. Do not perform this
procedure if the eyeball structure has been violated. If there is a penetrating globe injury,
apply a Fox shield for protection and seek immediate ophthalmic surgical support.
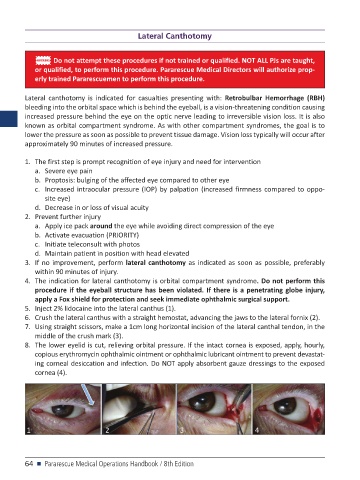
5. Inject 2% lidocaine into the lateral canthus (1).
6. Crush the lateral canthus with a straight hemostat, advancing the jaws to the lateral fornix (2).
7. Using straight scissors, make a 1cm long horizontal incision of the lateral canthal tendon, in the
middle of the crush mark (3).
8. The lower eyelid is cut, relieving orbital pressure. If the intact cornea is exposed, apply, hourly,
copious erythromycin ophthalmic ointment or ophthalmic lubricant ointment to prevent devastat-
ing corneal desiccation and infection. Do NOT apply absorbent gauze dressings to the exposed
cornea (4).
64 n Pararescue Medical Operations Handbook / 8th Edition