
Page 54 - PJ MED OPS Handbook 8th Ed
P. 54
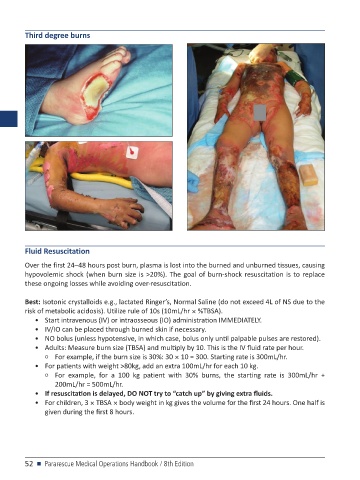
Third degree burns
Fluid Resuscitation
Over the first 24–48 hours post burn, plasma is lost into the burned and unburned tissues, causing
hypovolemic shock (when burn size is >20%). The goal of burn-shock resuscitation is to replace
these ongoing losses while avoiding over-resuscitation.
Best: Isotonic crystalloids e.g., lactated Ringer’s, Normal Saline (do not exceed 4L of NS due to the
risk of metabolic acidosis). Utilize rule of 10s (10mL/hr × %TBSA).
• Start intravenous (IV) or intraosseous (IO) administration IMMEDIATELY.
• IV/IO can be placed through burned skin if necessary.
• NO bolus (unless hypotensive, in which case, bolus only until palpable pulses are restored).
• Adults: Measure burn size (TBSA) and multiply by 10. This is the IV fluid rate per hour.
○ For example, if the burn size is 30%: 30 × 10 = 300. Starting rate is 300mL/hr.
• For patients with weight >80kg, add an extra 100mL/hr for each 10 kg.
○ For example, for a 100 kg patient with 30% burns, the starting rate is 300mL/hr +
200mL/hr = 500mL/hr.
• If resuscitation is delayed, DO NOT try to “catch up” by giving extra fluids.
• For children, 3 × TBSA × body weight in kg gives the volume for the first 24 hours. One half is
given during the first 8 hours.
52 n Pararescue Medical Operations Handbook / 8th Edition