
Page 52 - PJ MED OPS Handbook 8th Ed
P. 52
NOTES:
• Make a single attempt at laryngoscopy (cord visualization), if unable to visualize the cords
due to edema, proceed to surgical airway. If able to visualize the cords, make no more than 2
attempts at endotracheal intubation.
• Burns or explosions in a closed space are associated with higher risk of inhalation injury than
burns occurring in open areas.
• Supraglottic airway is not appropriate because edema will continue to increase over 48 hours
and these tubes do not overcome vocal-cord edema.
• Endotracheal tube must be secured circumferentially around the neck using cotton ties or
similar. Tape does not stick reliably in the field due to dirt, sweat, and nature of injury (facial
trauma/burns).
• Place nasogastric tube to decompress stomach in intubated patients.
• Perform frequent endotracheal suction of intubated patients to ensure tube patency and
remove mucus/debris (approximately once an hour or more frequently if oxygen saturation
[SpO2] drops).
• If there is evidence of inhalation injury, use 3–5mL of endotracheal saline to facilitate suction-
ing and prevent tube inspissation and obstruction.
• Monitoring end-tidal CO2 is an important capability for all intubated patients. A rising end-
tidal CO2 could indicate clogging of endotracheal tube or poor ventilation from another
cause (e.g., bronchospasm, tight eschar across chest).
• Perform a surgical escharotomy of the chest for tight, circumferential, full-thickness burns
that impair breathing. Incision goes through the full thickness of the burn and into the fat.
Expect some pain and bleeding.
• Use bronchodilators (e.g., albuterol inhaler) for intubated patients with inhalation injury, if
available.
• Ventilator management of burn patients can be complicated and evolve as pulmonary con-
ditions change due to volume overload/edema and acute respiratory distress syndrome
(ARDS). Telemedicine consultation with skilled providers is recommended.
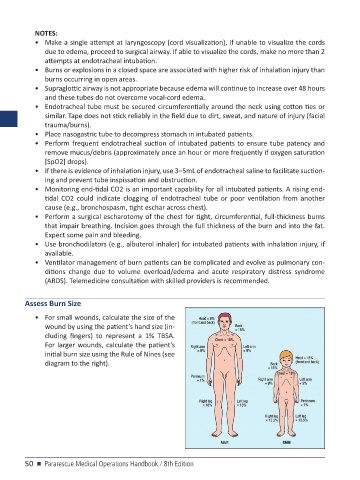
Assess Burn Size
• For small wounds, calculate the size of the
wound by using the patient’s hand size (in-
cluding fingers) to represent a 1% TBSA.
For larger wounds, calculate the patient’s
initial burn size using the Rule of Nines (see
diagram to the right).
50 n Pararescue Medical Operations Handbook / 8th Edition