
Page 46 - PJ MED OPS Handbook 8th Ed
P. 46
Procedure:
1. Locate 4th or 5th intercostal space (approximately at the nipple level in males) just anterior to
the mid-axillary line on the affected side. Prep incision site with chlorhexidine (ChloraPrep) or
equivalent and don sterile gloves.
2. If the patient is conscious:
a. Perform procedural sedation and/or local anesthetic at incision site with 1% or 2% lidocaine.
b. Holding the needle at a 90° angle to the skin, insert the needle down to the rib infiltrating
the periosteum of the rib.
c. Walk the needle up and over the top of the rib, injecting gently into the area of the pleura.
d. Disconnect needle from syringe and leave needle in place to mark injection site. Make in-
cision over it.
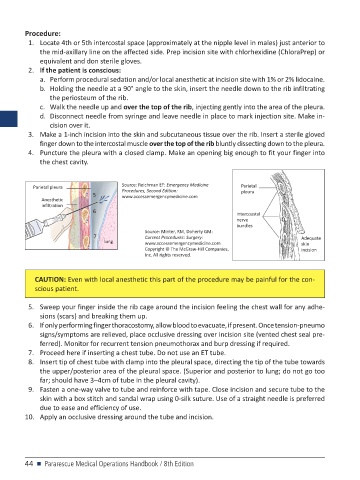
3. Make a 1-inch incision into the skin and subcutaneous tissue over the rib. Insert a sterile gloved
finger down to the intercostal muscle over the top of the rib bluntly dissecting down to the pleura.
4. Puncture the pleura with a closed clamp. Make an opening big enough to fit your finger into
the chest cavity.
Parietal pleura Source: Reichman EF: Emergency Medicine Parietal
Procedures, Second Edition:
5 www.accessemergencymedicine.com pleura
Anesthetic
infiltration
6 Intercoastal
nerve
bundles
Source: Minter, RM, Doherty GM:
7 Current Procedures: Surgery: Adequate
lung www.accessemergencymedicine.com skin
Copyright © The McGraw-Hill Companies, incision
Inc. All rights reserved.
CAUTION: Even with local anesthetic this part of the procedure may be painful for the con-
scious patient.
5. Sweep your finger inside the rib cage around the incision feeling the chest wall for any adhe-
sions (scars) and breaking them up.
6. If only performing finger thoracostomy, allow blood to evacuate, if present. Once tension-pneumo
signs/symptoms are relieved, place occlusive dressing over incision site (vented chest seal pre-
ferred). Monitor for recurrent tension pneumothorax and burp dressing if required.
7. Proceed here if inserting a chest tube. Do not use an ET tube.
8. Insert tip of chest tube with clamp into the pleural space, directing the tip of the tube towards
the upper/posterior area of the pleural space. (Superior and posterior to lung; do not go too
far; should have 3–4cm of tube in the pleural cavity).
9. Fasten a one-way valve to tube and reinforce with tape. Close incision and secure tube to the
skin with a box stitch and sandal wrap using 0-silk suture. Use of a straight needle is preferred
due to ease and efficiency of use.
10. Apply an occlusive dressing around the tube and incision.
44 n Pararescue Medical Operations Handbook / 8th Edition