
Page 81 - JSOM Summer 2024
P. 81
pneumothorax, and subcutaneous emphysema. An extended
focused assessment with sonography in trauma (E-FAST) was
performed and was initially negative. A secondary survey re-
vealed a catheter from a needle thoracostomy that was inserted
into the hub at the 4th ICS, just lateral to the sternal border. The
catheter had been previously connected to extension tubing that
was filled with blood and clamped prior to arrival. Temporary
unclamping of the tubing revealed a pulsatile flow of blood,
concerning for cardiac or great vessel injury. With stable vital
signs, the patient was sent for computed tomography angiogra-
phy (CTA) of the chest, abdomen, and pelvis. The CTA revealed FIGURE 2 14-gauge angiocatheter
that the catheter traversed the right ventricle and interventricu- after removal.
lar septum and terminated in the left ventricle (Figure 1).
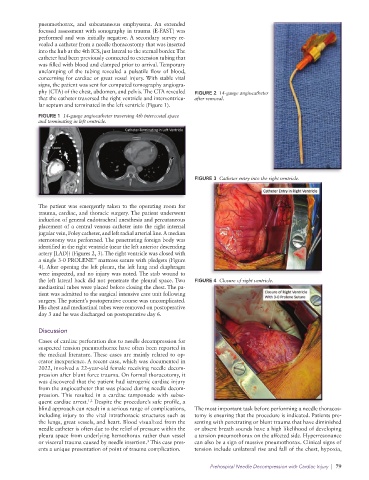
FIGURE 1 14-gauge angiocatheter traversing 4th intercostal space
and terminating in left ventricle.
FIGURE 3 Catheter entry into the right ventricle.
The patient was emergently taken to the operating room for
trauma, cardiac, and thoracic surgery. The patient underwent
induction of general endotracheal anesthesia and percutaneous
placement of a central venous catheter into the right internal
jugular vein, Foley catheter, and left radial arterial line. A median
sternotomy was performed. The penetrating foreign body was
identified in the right ventricle (near the left anterior descending
artery [LAD]) (Figures 2, 3). The right ventricle was closed with
™
a single 3-0 PROLENE mattress suture with pledgets (Figure
4). After opening the left pleura, the left lung and diaphragm
were inspected, and no injury was noted. The stab wound to
the left lateral back did not penetrate the pleural space. Two FIGURE 4 Closure of right ventricle.
mediastinal tubes were placed before closing the chest. The pa-
tient was admitted to the surgical intensive care unit following
surgery. The patient’s postoperative course was uncomplicated.
His chest and mediastinal tubes were removed on postoperative
day 3 and he was discharged on postoperative day 6.
Discussion
Cases of cardiac perforation due to needle decompression for
suspected tension pneumothorax have often been reported in
the medical literature. These cases are mainly related to op-
erator inexperience. A recent case, which was documented in
2022, involved a 22-year-old female receiving needle decom-
pression after blunt force trauma. On formal thoracotomy, it
was discovered that the patient had iatrogenic cardiac injury
from the angiocatheter that was placed during needle decom-
pression. This resulted in a cardiac tamponade with subse-
1,2
quent cardiac arrest. Despite the procedure’s safe profile, a
blind approach can result in a serious range of complications, The most important task before performing a needle thoracos-
including injury to the vital intrathoracic structures such as tomy is ensuring that the procedure is indicated. Patients pre-
the lungs, great vessels, and heart. Blood visualized from the senting with penetrating or blunt trauma that have diminished
needle catheter is often due to the relief of pressure within the or absent breath sounds have a high likelihood of developing
pleura space from underlying hemothorax rather than vessel a tension pneumothorax on the affected side. Hyperresonance
3
or visceral trauma caused by needle insertion. This case pres- can also be a sign of massive pneumothorax. Clinical signs of
ents a unique presentation of point of trauma complication. tension include unilateral rise and fall of the chest, hypoxia,
Prehospital Needle Decompression with Cardiac Injury | 79