
Page 113 - JSOM Summer 2023
P. 113
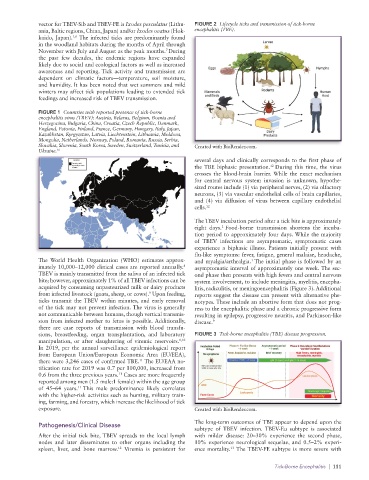
vector for TBEV-Sib and TBEV-FE is Ixodes pesculatus (Lithu- FIGURE 2 Lifecycle ticks and transmission of tick-borne
ania, Baltic regions, China, Japan) and/or Ixodes ovatus (Hok- encephalitis (TBE).
1,6
kaido, Japan). The infected ticks are predominantly found
in the woodland habitats during the months of April through
7
November with July and August as the peak months. During
the past few decades, the endemic regions have expanded
likely due to social and ecological factors as well as increased
awareness and reporting. Tick activity and transmission are
dependent on climatic factors—temperature, soil moisture,
and humidity. It has been noted that wet summers and mild
winters may affect tick populations leading to extended tick
feedings and increased risk of TBEV transmission.
FIGURE 1 Countries with reported presence of tick-borne
encephalitis virus (TBEV): Austria, Belarus, Belgium, Bosnia and
Herzegovina, Bulgaria, China, Croatia, Czech Republic, Denmark,
England, Estonia, Finland, France, Germany, Hungary, Italy, Japan,
Kazakhstan, Kyrgyzstan, Latvia, Liechtenstein, Lithuania, Moldova,
Mongolia, Netherlands, Norway, Poland, Romania, Russia, Serbia,
Slovakia, Slovenia, South Korea, Sweden, Switzerland, Tunisia, and Created with BioRender.com.
Ukraine. 16
several days and clinically corresponds to the first phase of
the TBE biphasic presentation. During this time, the virus
12
crosses the blood-brain barrier. While the exact mechanism
for central nervous system invasion is unknown, hypothe-
sized routes include (1) via peripheral nerves, (2) via olfactory
neurons, (3) via vascular endothelial cells of brain capillaries,
and (4) via diffusion of virus between capillary endothelial
cells. 12
The TBEV incubation period after a tick bite is approximately
1
eight days. Food-borne transmission shortens the incuba-
tion period to approximately four days. While the majority
of TBEV infections are asymptomatic, symptomatic cases
experience a biphasic illness. Patients initially present with
flu-like symptoms: fever, fatigue, general malaise, headache,
The World Health Organization (WHO) estimates approx- and myalgia/arthralgia. The initial phase is followed by an
1
imately 10,000–12,000 clinical cases are reported annually. asymptomatic interval of approximately one week. The sec-
8
TBEV is mainly transmitted from the saliva of an infected tick ond phase then presents with high fevers and central nervous
bite; however, approximately 1% of all TBEV infections can be system involvement, to include meningitis, myelitis, encepha-
acquired by consuming unpasteurized milk or dairy products litis, radiculitis, or meningoencephalitis (Figure 3). Additional
from infected livestock (goats, sheep, or cows). Upon feeding, reports suggest the disease can present with alternative phe-
9
ticks transmit the TBEV within minutes, and early removal notypes. These include an abortive form that does not prog-
of the tick may not prevent infection. The virus is generally ress to the encephalitic phase and a chronic progressive form
not communicable between humans, though vertical transmis- resulting in epilepsy, progressive neuritis, and Parkinson-like
sion from infected mother to fetus is possible. Additionally, disease. 9
there are case reports of transmission with blood transfu-
sions, breastfeeding, organ transplantation, and laboratory FIGURE 3 Tick-borne encephalitis (TBE) disease progression.
manipulation, or after slaughtering of viremic reservoirs. 1,10
In 2019, per the annual surveillance epidemiological report
from European Union/European Economic Area (EU/EEA),
11
there were 3,246 cases of confirmed TBE. The EU/EAA no-
tification rate for 2019 was 0.7 per 100,000, increased from
0.6 from the three previous years. Cases are more frequently
11
reported among men (1.5 male:1 female) within the age group
of 45–64 years. This male predominance likely correlates
11
with the higher-risk activities such as hunting, military train-
ing, farming, and forestry, which increase the likelihood of tick
exposure. Created with BioRender.com.
The long-term outcomes of TBE appear to depend upon the
Pathogenesis/Clinical Disease
subtype of TBEV infection. TBEV-Eu subtype is associated
After the initial tick bite, TBEV spreads to the local lymph with milder disease: 20–30% experience the second phase,
nodes and later disseminates to other organs including the 10% experience neurological sequelae, and 0.5–2% experi-
12
spleen, liver, and bone marrow. Viremia is persistent for ence mortality. The TBEV-FE subtype is more severe with
13
Tick-Borne Encephalitis | 111