
Page 142 - JSOM Winter 2021
P. 142
mortality in abdominally wounded patients was usually due 2. What are the preventable causes of death in abdominal in-
to hemorrhage. Concomitant head injury, 3 or more injured jury and abdominal evisceration specifically?
intraabdominal organs, and delayed presentation (defined as In the past, the recommendations in the TCCC Guidelines
greater than 12 hours from time of injury) were associated with for casualties with penetrating abdominal trauma have fo-
mortality. Small intestine 69 (63.3%), colon 48 (44%), and cused primarily on preventing death due to abdominopelvic
liver 41 (37.6%) were the most commonly injured organs. In hemorrhage, since that is the primary cause of preventable
this series, abdominally wounded patients required an average death in casualties with this type of wound. An estimated
of 2100mL of blood products to restore hemodynamic stabil- two-thirds of deaths involving war- related abdominal evis-
7
ity. Death after 48 hours was almost universally due to sepsis. 17 ceration are due to hemorrhage. It is unclear whether the
presence of eviscerated abdominal contents should result
in any alteration of TCCC recommendations regarding the
management of noncompressible sources of hemorrhage,
but the presence of a source of bleeding that is visible as
a result of the evisceration does offer the potential to use
a CoTCCC-recommended hemostatic dressing to control
that source of bleeding. Infection is also a potentially pre-
ventable cause of death in eviscerating injuries, with sepsis
causing death in an estimated 25% of combat wounded
7
abdominal trauma patients. Finally, an estimated 15–25%
of patients with eviscerating injury will have associated
thoracic injuries. 7,20 Thoracic injuries that produce open or
tension pneumothoraces should be managed in accordance
with TCCC recommendations for those conditions.
3. What prehospital interventions reduce the mortality of ab-
dominal evisceration?
Treatment for any noncompressible hemorrhage must re-
main the primary consideration in the prehospital manage-
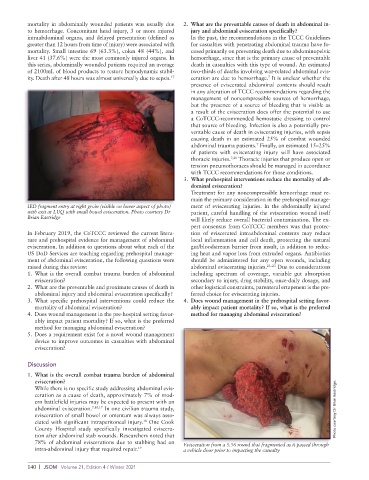
IED fragment entry at right groin (visible on lower aspect of photo) ment of eviscerating injuries. In the abdominally injured
with exit at LUQ with small bowel evisceration. Photo courtesy Dr patient, careful handling of the evisceration wound itself
Brian Eastridge will likely reduce overall bacterial contamination. The ex-
pert consensus from CoTCCC members was that protec-
In February 2019, the CoTCCC reviewed the current litera- tion of eviscerated intraabdominal contents may reduce
ture and prehospital evidence for management of abdominal local inflammation and cell death, protecting the natural
evisceration. In addition to questions about what each of the gut/bloodstream barrier from insult, in addition to reduc-
US DoD Services are teaching regarding prehospital manage- ing heat and vapor loss from extruded organs. Antibiotics
ment of abdominal evisceration, the following questions were should be administered for any open wounds, including
raised during this review: abdominal eviscerating injuries. 21–23 Due to considerations
1. What is the overall combat trauma burden of abdominal including spectrum of coverage, variable gut absorption
evisceration? secondary to injury, drug stability, once-daily dosage, and
2. What are the preventable and proximate causes of death in other logistical constraints, parenteral ertapenem is the pre-
abdominal injury and abdominal evisceration specifically? ferred choice for eviscerating injuries.
3. What specific prehospital interventions could reduce the 4. Does wound management in the prehospital setting favor-
mortality of abdominal evisceration? ably impact patient mortality? If so, what is the preferred
4. Does wound management in the pre-hospital setting favor- method for managing abdominal evisceration?
ably impact patient mortality? If so, what is the preferred
method for managing abdominal evisceration?
5. Does a requirement exist for a novel wound management
device to improve outcomes in casualties with abdominal
evisceration?
Discussion
1. What is the overall combat trauma burden of abdominal
evisceration?
While there is no specific study addressing abdominal evis-
ceration as a cause of death, approximately 7% of mod-
ern battlefield injuries may be expected to present with an
abdominal evisceration. 7,10,17 In one civilian trauma study, Photo courtesy Dr Brian Eastridge.
evisceration of small bowel or omentum was always asso-
18
ciated with significant intraperitoneal injury. One Cook
County Hospital study specifically investigated eviscera-
tion after abdominal stab wounds. Researchers noted that
78% of abdominal eviscerations due to stabbing had an Evisceration from a 5.56 round that fragmented as it passed through
intra-abdominal injury that required repair. 19 a vehicle door prior to impacting the casualty
140 | JSOM Volume 21, Edition 4 / Winter 2021