
Page 89 - 2020 JSOM Winter
P. 89
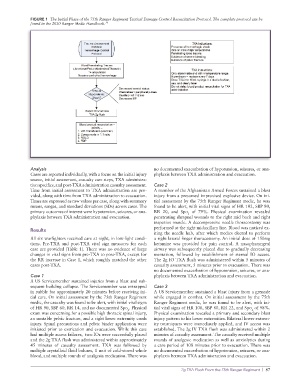
FIGURE 1 The Initial Phase of the 75th Ranger Regiment Tactical Damage Control Resuscitation Protocol. The complete protocol can be
found in the 2020 Ranger Medic Handbook. 17
Analysis no documented exacerbation of hypotension, seizures, or ana-
Cases are reported individually, with a focus on the initial injury phylaxis between TXA administration and evacuation.
source, initial assessment, casualty care steps, TXA administra-
tion specifics, and post-TXA administration casualty assessment. Case 2
Time from initial assessment to TXA administration are pro- A member of the Afghanistan Armed Forces sustained a blast
vided, along with time from TXA administration to evacuation. injury from a presumed improvised explosive device. On ini-
Times are expressed as raw values per case, along with summary tial assessment by the 75th Ranger Regiment medic, he was
means, ranges, and standard deviations (SDs) across cases. The found to be alert, with initial vital signs of HR 102, SBP 80,
primary outcomes of interest were hypotension, seizures, or ana- RR 20, and Spo of 79%. Physical examination revealed
2
phylaxis between TXA administration and evacuation. penetrating shrapnel wounds to the right mid back and right
trapezius muscle. A decompressive needle thoracostomy was
Results performed at the right midaxillary line. Blood was noticed ex-
iting the needle hub, after which medics elected to perform
All six warfighters received care at night, in low-light condi- a right lateral finger thoracostomy. An initial dose of 150mg
tions. Pre-TXA and post-TXA vital sign measures for each ketamine was provided for pain control. A nasopharyngeal
case are provided (Table 1). There was no evidence of large airway was subsequently placed due to gradually decreasing
changes in vital signs from pre-TXA to post-TXA, except for mentation, followed by establishment of sternal IO access.
the RR increase in Case 1, which roughly matched the other The 2g IO TXA flush was administered within 5 minutes of
cases post-TXA. casualty assessment, 5 minutes prior to evacuation. There was
no documented exacerbation of hypotension, seizures, or ana-
Case 1 phylaxis between TXA administration and evacuation.
A US Servicemember sustained injuries from a blast and sub-
sequent building collapse. The Servicemember was entrapped Case 3
in rubble for approximately 20 minutes before receiving ini- A US Servicemember sustained a blast injury from a grenade
tial care. On initial assessment by the 75th Ranger Regiment while engaged in combat. On initial assessment by the 75th
medic, the casualty was found to be alert, with initial vital signs Ranger Regiment medic, he was found to be alert, with ini-
of HR 90, SBP 60, RR 14, and no documented Spo . Physical tial vital signs of HR 100, SBP 80, RR 22, and Spo of 98%.
2
2
exam was concerning for a possible high thoracic spinal injury, Physical examination revealed a primary and secondary blast
an unstable pelvic fracture, and a right lower extremity crush injury pattern to his lower extremities. Bilateral lower extrem-
injury. Spinal precautions and pelvic binder application were ity tourniquets were immediately applied, and IV access was
initiated prior to extrication and evacuation. While this case established. The 2g IV TXA flush was administered within 2
had multiple access failures, two IOs were successfully placed minutes of casualty assessment. The casualty received multiple
and the 2g TXA flush was administered within approximately rounds of analgesic medication as well as anxiolytics during
45 minutes of casualty assessment. TXA was followed by a care period of 108 minutes prior to evacuation. There was
multiple crystalloid fluid boluses, 1 unit of cold-stored whole no documented exacerbation of hypotension, seizures, or ana-
blood, and multiple rounds of analgesia medication. There was phylaxis between TXA administration and evacuation.
2g TXA Flush From the 75th Ranger Regiment | 87