
Page 58 - 2020 JSOM Winter
P. 58
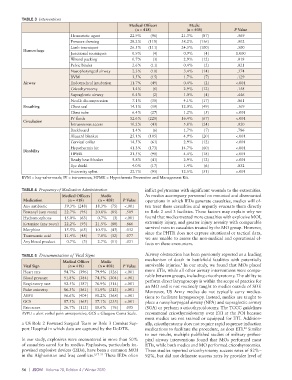
TABLE 3 Interventions
Medical Officers Medic
(n = 418) (n = 408) P Value
Hemostatic agent 22.9% (96) 21.3% (87) .569
Pressure dressing 28.2% (118) 38.2% (156) .002
Limb tourniquet 26.5% (111) 24.5% (100) .500
Hemorrhage
Junctional tourniquet 0.9% (4) 0.9% (4) 1.000
Wound packing 0.7% (3) 2.9% (12) .018
Pelvic binder 2.6% (11) 0.4% (2) .021
Nasopharyngeal airway 2.3% (10) 3.4% (14) .374
BVM 3.5% (15) 1.7% (7) .129
Airway Endotracheal intubation 11.7% (49) 0.4% (2) <.001
Cricothyrotomy 1.4% (6) 2.9% (12) .158
Supraglottic airway 0.4% (2) 1.0% (4) .446
Needle decompression 7.1% (30) 4.1% (17) .061
Breathing Chest seal 14.1% (59) 12.0% (49) .369
Chest tube 6.4% (27) 1.2% (5) <.001
IV fluids 52.6% (220) 16.4% (67) <.001
Circulation
Intraosseous access 10.2% (43) 5.8% (24) .020
Backboard 1.4% (6) 1.7% (7) .786
Blizzard blanket 25.1% (105) 4.9% (20) <.001
Cervical collar 14.5% (61) 2.9% (12) <.001
Hypothermia kit 41.3% (173) 14.7% (60) <.001
Disability
HPMK 21.5% (90) 4.4% (18) <.001
Ready heat blanket 9.8% (41) 2.9% (12) <.001
Eye shield 4.0% (17) 1.4% (6) .032
Extremity splint 22.7% (95) 12.5% (51) <.001
BVM = bag-valve-mask; IV = intravenous; HPMK = Hypothermia Prevention and Management Kit.
TABLE 4 Frequency of Medication Administration inflict polytrauma with significant wounds to the extremities.
Medical Officers Medic As medics accompany personnel on mounted and dismounted
Medication (n = 418) (n = 408) P Value operations in which IEDs generate casualties, medics will of-
Any antibiotic 59.3% (248) 18.3% (75) <.001 ten treat these casualties and urgently evacuate them directly
Fentanyl (any route) 22.7% (95) 20.8% (85) .509 to Role 2 and 3 facilities. These factors may explain why we
Hydromorphone 15.0% (63) 0.7% (3) <.001 found that medics treated more casualties with explosive MOI,
Ketamine (any route) 22.2% (93) 21.5% (88) .866 extremity injury, and greater injury severity with comparable
Morphine 15.5% (65) 10.5% (43) .032 survival rates to casualties treated by the MO group. However,
since the PHTR does not capture situational or tactical data,
Tranexamic acid 11.4% (48) 7.8% (32) .077 we are unable to assess the non-medical and operational ef-
Any blood product 0.7% (3) 2.7% (11) .031
fects on these encounters.
TABLE 5 Documentation of Vital Signs Airway obstruction has been previously reported as a leading
Medical Officer Medic mechanism of death in battlefield fatalities with potentially
5
Vital Sign (n = 418) (n = 408) P Value survivable injuries. In our study, we found that MOs placed
Heart rate 94.7% (396) 79.9% (326) <.001 more ETIs, while all other airway interventions were compa-
Blood pressure 91.8% (384) 74.5% (304) <.001 rable between groups, including cricothyrotomy. The ability to
perform direct laryngoscopy is within the scope of practice for
Respiratory rate 92.5% (387) 76.9% (314) <.001 an MO and is not routinely taught to medics outside of SOF.
Pulse oximetry 86.3% (361) 51.9% (212) <.001 Moreover, US Army medics do not typically carry medica-
AVPU 96.6% (404) 90.2% (368) <.001 tions to facilitate laryngoscopy. Instead, medics are taught to
GCS 87.3% (365) 57.1% (233) <.001 place a nasopharyngeal airway (NPA) and supraglottic airway
Pain score 26.7% (112) 18.6% (76) .005 (SGA) or perform a cricothyroidotomy. The TCCC guidelines
AVPU = alert verbal pain unresponsive; GCS = Glasgow Coma Scale. recommend cricothyroidotomy over ETI at the POI because
most medics are not trained or equipped for ETI. Addition-
a US Role 2 Forward Surgical Team or Role 3 Combat Sup- ally, cricothyrotomy does not require rapid sequence induction
port Hospital in which data are captured by the DoDTR. medications to facilitate the procedure, as does ETI. Similar
22
to our results, multiple published studies of military prehos-
In our study, explosives were encountered in more than 50% pital airway interventions found that MOs performed most
of casualties cared for by medics. Explosives, particularly im- ETIs, while both medics and MO performed cricothyrotomies.
provised explosive devices (IEDs), have been a common MOI These studies reported cricothyrotomy success rates of 82%–
in the Afghanistan and Iraq conflicts. 5,17–21 These IEDs often 92%, but did not delineate success rates by provider level of
56 | JSOM Volume 20, Edition 4 / Winter 2020