
Page 57 - 2020 JSOM Winter
P. 57
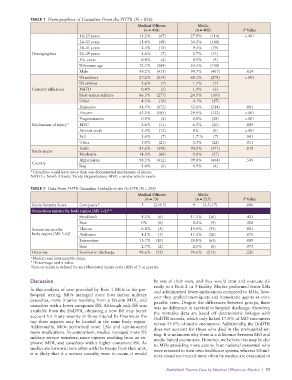
TABLE 1 Demographics of Casualties From the PHTR (N = 826)
Medical Officers Medic
(n = 418) (n = 408) P Value
18–25 years 11.2% (47) 27.9% (114) <.001
26–33 years 11.4% (48) 34.3% (140)
34–41 years 2.3% (10) 9.5% (39)
Demographics 42–49 years 1.6% (7) 2.7% (11)
50+ years 0.4% (2) 0.9% (4)
Unknown age 72.7% (304) 24.5% (100)
Male 99.2% (415) 99.7% (407) .624
US military 27.2% (114) 68.1% (278) <.001
US civilian 1.6% (7) 1.7% (7)
Casualty affiliation NATO 0.4% (2) 1.4% (6)
Host-nation military 66.3% (277) 24.5% (100)
Other 4.3% (18) 4.1% (17)
Explosive 41.5% (172) 52.4% (214) .001
Firearm 45.2% (189) 29.9% (122) <.001
Fragmentation 0.9% (4) 6.8% (28) <.001
Mechanism of injury* MVC 2.6% (11) 6.3% (26) .009
Aircraft crash 2.9% (12) 0% (0) <.001
Fall 1.6% (7) 1.7.% (7) .963
Other 5.0% (21) 5.3% (22) .811
Battle 85.6% (358) 90.9% (371) .018
Battle status
Nonbattle 14.3% (60) 9.0% (37)
Afghanistan 98.5% (412) 99.0% (404) .549
Country
Iraq 1.4% (6) 0.9% (4)
*Casualties could have more than one documented mechanism of injury.
NATO = North Atlantic Treaty Organization; MVC = motor vehicle crash.
TABLE 2 Data From PHTR Casualties Linkable to the DoDTR (N = 298)
Medical Officers Medic
(n = 73) (n = 225) P Value
Injury Severity Score Composite* 5 (2–9.5) 9 (3.5–17) .006
Nonserious injuries by body region (AIS 1–2)**
Head/neck 8.2% (6) 11.5% (26) .423
Face 0% (0) 0.4% (9) .568
Serious injuries by Thorax 6.8% (5) 14.6% (33) .081
body region (AIS 3–6) † Abdomen 4.1% (3) 11.5% (26) .070
Extremities 13.7% (10) 28.8% (65) .009
Skin 2.7% (2) 2.6% (6) .973
Outcome Survival to discharge 98.6% (72) 95.6% (215) .226
*Median and interquartile range.
**Percentage and n value.
† Serious injury is defined by an abbreviated injury scale (AIS) of 3 or greater.
Discussion be one of their own, and they would treat and evacuate di-
rectly to a Role 2 or 3 facility. Medics performed fewer LSIs
In this analysis of care provided by Role 1 MOs in the pre- and administered fewer medications compared to MOs, how-
hospital setting, MOs managed more host nation military ever they applied tourniquets and hemostatic agents at com-
casualties, more injuries resulting from a firearm MOI, and parable rates. Despite the differences between groups, there
casualties with a lower composite ISS. Although only ISS was was no difference in survival to hospital discharge. However,
available from the DoDTR, obtaining a new ISS may better the mortality data are based off deterministic linkages with
account for injury severity in those injured by firearm as the DoDTR records, which only linked 17.0% of MO encounters
top three injuries may be located in the same body region. versus 55.0% of medic encounters. Additionally, the DoDTR
Additionally, MOs performed more LSIs and administered does not account for those who died in the prehospital set-
more medications. In comparison, medics managed more US ting. It is unknown why there is a difference between MO and
military service members, more injuries resulting from an ex- medic-linked encounters. However, we believe this may be due
plosive MOI, and casualties with a higher composite ISS. As to MOs providing more care to host national personnel who
medics are forward more often with the troops from their unit, were returned to their own healthcare system, whereas US mil-
it is likely that if a serious casualty were to occur, it would
itary casualties treated more often by medics are evacuated to
Battlefield Trauma Care by Medical Officers vs. Medics | 55