
Page 145 - JSOM Fall 2020
P. 145
Synchronous (real-time continuous) telemedicine using Positioning of the patient to help clear airway obstruction
video or remote patient monitoring systems should be considered first, when possible. The simple option of
placing the patient in a sitting position, placing the patient in
Monitoring is the active process of assessing the patient the lateral “recovery” position, or head tilt-chin lift/jaw thrust
throughout a procedure. It involves the gathering, document- maneuver may be enough to ensure adequate respirations.
ing and interpretation of vital signs and other data, and the
continuous assessment of their clinical status. Telemedicine Simple adjuncts such as a nasal or oropharyngeal airway (in
can be an important adjunct and critical capability to employ an unconscious patient) may be utilized in addition to proper
when monitoring a patient undergoing complex procedures. positioning to help ensure a clear airway.
AIRWAY For those patients requiring active airway assistance, the first
• Minimum: Medic is prepared for a ketamine step should be inserting an NPA to open the airway. BVM
cricothyroidotomy. ventilation is the next step in the algorithm and though it ap-
• Better: Add ability to provide continuous sedation. pears to be relatively simple, the procedure requires prepara-
• Best: Add a responsible rapid-sequence intubation capa- tion, training, and skill to perform correctly. A spontaneously
bility (to include chemical paralysis) with airway main- breathing patient may prove challenging, but properly deliv-
tenance (to include suction) and continuous sedation. ered, synchronous breaths may be the only requirement to
assist a patient’s respirations. Care should be taken to ensure
Per the PFC Capabilities Position Paper, a definitive airway proper volume and rate of bag-delivered breath. One hand
requires control of the patient’s airway with an inflated cuff in should provide moderate pressure to the bag for no more than
the trachea. In addition, sedation is needed to keep the patient 50% of the volume of an adult bag or just enough to see the
comfortable and sustain the airway. 8 chest begin to rise at a rate of 12–16 breaths per minute (one
breath every 4–5 seconds) initially. It is important to avoid hy-
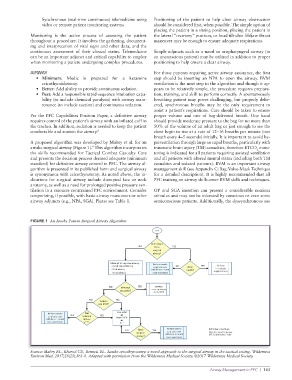
A proposed algorithm was developed by Mabry et al. for an perventilation through large or rapid breaths, particularly with
awake surgical airway (Figure 1). This algorithm incorporates traumatic brain injury (TBI) casualties, therefore ETCO moni-
9
2
the skills recommended for Tactical Combat Casualty Care toring is indicated for all patients requiring assisted ventilation
and presents the decision process deemed adequate (minimum and all patients with altered mental status (including both TBI
standard) for definitive airway control in PFC. The airway al- casualties and sedated patients). BVM is an important airway
gorithm is presented in its published form and surgical airway management skill (see Appendix C: Bag-Valve-Mask Technique
is synonymous with cricothyrotomy. As noted above, the in- for a detailed description). It is highly recommended that all
dications for surgical airway include disrupted face or neck PFC training on airway skills cover BVM skills and techniques.
anatomy, as well as a need for prolonged positive pressure ven-
tilation in a resource constrained PFC environment. Consider OP and SGA insertion can present a considerable noxious
temporizing, if possible, with basic airway maneuvers or other stimulus and may not be tolerated by conscious or even some
airway adjuncts (e.g., NPA, SGA). Please see Table 1. semiconscious patients. Additionally, the dyssynchronous use
FIGURE 1 An Awake Patient Surgical Airway Algorithm
start
Indications
NO for a YES
surgical
airway?
Attempt to improve airway: Perform awake
- Head repositioning surgical airway NO Near YES Perform
immediate
- Oral airway with ketamine and death? surgical airway
- Nasal airway local anesthesia
NO Effective YES Conduct
outcome? ongoing airway
assessment
NO YES
Able to
use BVM?
Perform awake NO Can YES Use BVM
or
surgical airway tolerate Insert SGA
with ketamine and SGA or or
local anesthesia ETT? ETT
NO Need YES Perform awake BVM: Bag Valve Mask
surgical airway
surgical with ketamine and SGA: Supraglottic Airway
airway? local anesthesia ETT: Endotracheal Tube
Source: Mabry RL, Kharod CU, Bennett BL. Awake cricothyrotomy: a novel approach to the surgical airway in the tactical setting. Wilderness
Environ Med. 2017;28(2S):S61-8. Adapted with permission from the Wilderness Medical Society. ©2017 Wilderness Medical Society.
Airway Management in PFC | 143