
Page 93 - JSOM Fall 2019
P. 93
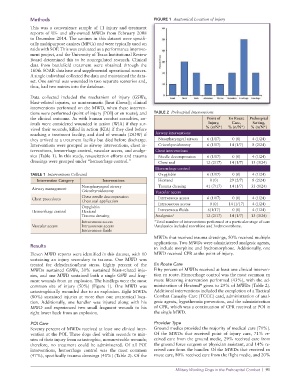
Methods FIGURE 1 Anatomical Location of Injury
This was a convenience sample of 11 injury and treatment
reports of US- and ally-owned MWDs from February 2008
to December 2014. The canines in this dataset were specifi-
cally multipurpose canines (MPCs) and were typically used on
raids with SOF. This was evaluated as a performance improve-
ment project, and the University of Texas Institutional Review
Board determined this to be nonregulated research. Clinical
data from battlefield treatment were obtained through the
160th SOAR database and supplemental operational sources.
A single individual collected the data and maintained the data-
set. One animal was wounded in two separate scenarios and,
thus, had two entries into the database.
Data collected included the mechanism of injury (GSWs,
blast-related injuries, or nontraumatic [heat illness]); clinical
interventions performed on the MWD, when these interven-
tions were performed (point of injury [POI] or en route); and TABLE 2 Prehospital Interventions
the clinical outcome. As with human combat casualties, an- Point of En Route Prehospital
imals were considered wounded in action (WIA) if they sur- Injury, Care, Setting,
vived their wounds, killed in action (KIA) if they died before % (n/N*) % (n/N*) % (n/N*)
reaching a treatment facility, and died of wounds (DOW) if Airway interventions
they arrived at a treatment facility but died before discharge. Nasopharyngeal airway 6 (1/17) 0 (0) 4 (1/24)
Interventions were grouped as airway interventions, chest in- Cricothyroidotomy 6 (1/17) 14 (1/7) 8 (2/24)
terventions, hemorrhage control, vascular access, and analge- Chest interventions
sics (Table 1). In this study, resuscitation efforts and trauma Needle decompression 6 (1/17) 0 (0) 4 (1/24)
dressings were grouped under “hemorrhage control.” Chest seal 12 (2/17) 14 (1/7) 13 (3/24)
Hemorrhage control
TABLE 1 Interventions Collected Oxyglobin 6 (1/17) 0 (0) 4 (1/24)
Intervention Category Interventions Hextend 0 (0) 29 (2/7) 8 (2/24)
Nasopharyngeal airway Trauma dressing 41 (7/17) 14 (1/7) 33 (8/24)
Airway management
Cricothyroidotomy Vascular access
Chest needle decompression
Chest procedures Intravenous access 6 (1/17) 0 (0) 4 (1/24)
Chest seal application Intraosseous access 0 (0) 14 (1/17) 4 (1/24)
Oxyglobin
Hemorrhage control Hextend Intravenous fluids 6(1/17) 0 (0) 4 (1/24)
Trauma dressing Analgesics † 12 (2/17) 14 (1/7) 13 (3/24)
Intravenous access *Total number of interventions performed at a particular stage of care
Vascular access Intraosseous access † Analgesics included morphine and hydromorphone.
Intravenous fluids
MWDs that received trauma dressings, 50% received multiple
applications. Two MWDs were administered analgesic agents,
Results to include morphine and hydromorphone. Additionally, one
Eleven MWD reports were identified in this dataset, with 10 MWD received CPR at the point of injury.
sustaining an injury secondary to trauma. One MWD was
treated for dehydration/heat stress. Eighty percent of the En Route Care
MWDs sustained GSWs, 30% sustained blast-related inju- Fifty percent of MWDs received at least one clinical interven-
ries, and one MWD sustained both a single GSW and frag- tion en route. Hemorrhage control was the most common en
ment wounds from an explosion. The hindlegs were the most route lifesaving intervention performed (43%), with the ad-
®
common site of injury (50%) (Figure 1). One MWD was ministration of Hextend given to 29% of MWDs (Table 2).
catastrophically wounded due to an explosion. Eight MWDs Additional interventions included the completion of a Tactical
(80%) sustained injuries at more than one anatomical loca- Combat Casualty Care (TCCC) card, administration of anal-
tion. Additionally, one handler was injured along with his gesic agents, hypothermia prevention, and the administration
MWD and experienced two small fragment wounds to his of CPR, which was a continuation of CPR received at POI in
right lower back from an explosion. the single MWD.
POI Care Provider Type
Seventy percent of MWDs received at least one clinical inter- Ground medics provided the majority of medical care (71%).
vention at the POI. Three dogs died within seconds to min- Of the MWDs that received point of injury care, 71% re-
utes of their injury from catastrophic, nonsurvivable wounds; ceived care from the ground medic, 29% received care from
therefore, no treatment could be administered. Of all POI the ground force surgeon or physician assistant, and 14% re-
interventions, hemorrhage control was the most common ceived care from the handler. Of the MWDs that received en
(47%), specifically trauma dressings (41%) (Table 2). Of the route care, 80% received care from the flight medic, and 20%
Military Working Dogs in the Prehospital Combat | 91