
Page 30 - JSOM Fall 2019
P. 30
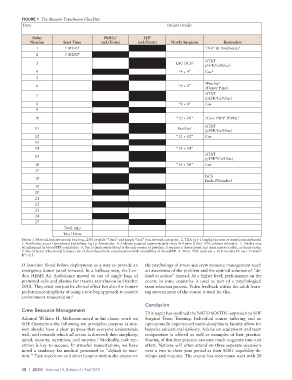
FIGURE 1 The Massive Transfusion Checklist.
Date: Patient Details
Bolus PRBCs 1 FFP 1
Number Start Time (mL/Units) (mL/Units) Notify Surgeons Reminders
1 ? MERT TXA & Antibiotics 3
2
2 ? MERT
iSTAT
3 LSG DCS?
pH/K/Ca/Gluc)
4 “4 + 4” Ca+ 4
5
?Futility
5
6 “6 + 6”
?Donor Panel
iSTAT
7
(pH/K/Ca/Gluc)
8 “8 + 8” Ca+
9
10 “10 + 10” ?Give FWB ?FVIIa 7
6
11 Futility? iSTAT
(pH/K/Ca/Gluc)
12 “12 + 12” Ca+
13
14 “14 + 14”
iSTAT
15
8
(pH/K /Ca/Gluc)
16 “16 + 16” Ca+
17
DCS
18
Ended/Transfer?
19
20
21
22
23
24
25
Total mLs
Total Units
Notes: 1. Note mL boluses in each box (e.g., 250) or circle “Units” and simply “tick” box for each unit given. 2. TXA 1g (~15mg/kg) as soon as transfusion indicated.
3. Antibiotics as per Operational Guidelines. Eg Co-Amoxiclav. 4. Calcium required approximately every 4+4 units (10mL 10% calcium chloride). 5. Futility may
be influenced by blood/FFP availability. 6. Use of fresh whole blood is the only source of platelets. lt requires a donor panel and takes time to collect, so decide early.
7. Use of factor VIIa should balance risk of thromboembolic complications with availability of blood/FFP. 8. 50mL 50% dextrose + 10 IU insulin IV over 15 min if
+
K >5.5.
O low-titer blood before deployment as a way to provide an the psychology of stress and crew resource management teach
emergency donor panel forward. In a halfway step, the Lon- an awareness of the problem and the optimal solution of “de-
don HEMS Air Ambulance moved to use of single bags of fault to action” instead. At a higher level, performance on the
premixed cells and plasma for trauma transfusion in October course in some countries is used as part of a psychological
2018. They cited not just its clinical effect but also the human team selection process. Video feedback within the adult learn-
performance simplicity of using a one-bag approach to austere ing environment of the course is used for this.
environment resuscitation. 6
Conclusion
Crew Resource Management
This paper has outlined the NATO SOSTDC approach to SOF
Admiral William H. McRaven noted in his classic work on Surgical Team Training. Individual course tailoring and an
SOF Operations the following six principles: purpose (a mis- operationally experienced multi-disciplinary faculty allow for
sion should have a clear purpose that everyone understands bespoke educational delivery. Advice on equipment and team
well, and towards which all action is directed) then simplicity, composition is offered as well as examples of best practice.
speed, security, repetition, and surprise. Medically, task rep- Sharing of this best practice can save much nugatory time and
7
etition is key to success. In stressful resuscitations, we have effort. Nations will often attend on three separate occasions
noted a tendency for medical personnel to “default to inac- over a two to three year period as their SOST capability de-
tion.” Task repetition and short lectures within the course on velops and matures. The course has seen teams start with 20
28 | JSOM Volume 19, Edition 3 / Fall 2019